Tobacco as Global Health Risk Factor: Disease Burden, Preventive Action and Regulatory Challenges

Tobacco use causes addiction and is a risk factor for the development of various noncommunicable diseases (NCDs). It is the only legal product that kills up to half of its consumers when used as intended by its manufacturer with an estimated 100 million people killed in the twentieth century and a further one billion set to be killed in the twenty- first century at annual cost to the global economy of approximately US$1.4 trillion. The tobacco epidemic’s toll is projected, in the twenty- first century, to fall overwhelmingly upon low-and-middle income (LMICs) countries that can afford it least. At the heart of the tobacco epidemic and its spread to LMICs is the steady globalisation of negative commercial determinants of health via the vector of this epidemic, the tobacco industry. At the heart of the epidemic’s prevention, conversely, are the evidence-based strategies available to government to counteract tobacco industry influence, shift the commercial determinants of health, and reduce demand for tobacco. To give impetus and coherence to national tobacco control efforts, the WHO Framework Convention on Tobacco Control (WHO FCTC) was adopted by the World Health Assembly and ratified by 182 countries to transform tobacco control best practices into legally binding and intergovernmental supported obligations. The principal challenge in global tobacco control is that of ensuring the WHO FCTC and its related Protocol on Illicit Trade remains impactful. WHO’s focus on scaling the WHO FCTC demand-reduction measures via implementation of the MPOWER technical package has reduced tobacco use prevalence and saved lives. This is being achieved through support provided to governments in the implementation of multisectoral tobacco control measures by intergovernmental organisations and civil society, but requires constant adaption to counteract evolving tobacco industry interference.
Introduction
The tobacco epidemic’s globalisation marks one of public health’s greatest challenges: lives lost, economies damaged, and developmental opportunities squandered due to the failure to earlier overcome industry’s scientific chicanery and political scare tactics. As the tobacco epidemic began to break over low- and middle-income countries (LMICs) – in the 1970s through to the 1990s – the responsive globalization of tobacco control efforts marked one of public health’s greatest triumphs in the early twenty-first century: the negotiation, creation, and implementation of the legally binding WHO Framework Convention on Tobacco Control (WHO FCTC) and its Protocol on Illicit Trade. Exposure to tobacco, including through second-hand smoke, caused 100 million deaths in the twentieth century. It is now the cause of eight million deaths annually and is projected to cause one billion deaths in the twenty-first century (WHO and NCI 2016; WHO 2019a).
At the heart of this ongoing tragedy and also the playbook by which it is being combatted is the steady globalisation of negative commercial determinants of health (Bettcher et al. 2000). These, the commercial determinants of health, are the “strategies and approaches used by the private sector to promote products and choices that are detrimental to health” (Kickbusch et al. 2016). Corporate influence over people, their environments, and their governments has deepened and extended to the detriment of health over the last century-and-a-half. Transnational tobacco corporations (TTCs) were a forerunner in deploying techniques for shaping the commercial determinants of health that later came to also characterise the food and beverage industries. The unhealthy consumption foisted on our world as a result is a significant contributor to noncommunicable diseases (NCDs) – the world’s leading cause of death, see Box 1 below – 41 million deaths annually or 70% of global mortality (WHO 2018a).
Box 1: NCDs and NCD Risk Factors
NCDs, unlike communicable diseases, are not transmitted by other people or by animals. Patterns of consumption, behaviour, and environmental exposure causatively linked with NCDs are known as NCD risk factors. Tobacco use is a leading risk factor for the development of NCDs. Tobacco use is joined by unhealthy diets, harmful alcohol use, physical inactivity, and air pollution in contributing to over two-thirds of death from NCDs (or approximately half of all mortality).
In 2011, the United Nations General Assembly Heads of State issued a political declaration committing the world to addressing the four leading risk factors for the four leading NCDs. This call for action on unhealthy diets, tobacco use, harmful alcohol use, and physical inactivity aims to prevent death and disability from cardiovascular diseases, cancer, chronic respiratory diseases, and diabetes. In 2016, 71% of total deaths were caused by NCDs, and 57%, over 32 million, were caused by just these four leading NCDs – see Fig. 1 below (WHO 2018a). In 2018, a subsequent meeting of the UN General Assembly Heads of State resulted in a new political declaration that added a new risk factor, air pollution, and a new NCD, mental/neurological conditions (UN Interagency Taskforce 2020). The 5 priority risk factors and NCDs are listed below (Fig. 1).
Human exposure to these NCD factors will be reduced through political action to promote healthy choices and environments (Moodie et al. 2013). As noted above, this will require efforts to address the commercial determinants of health by offsetting corporate influence over choices and environments, which will require action to prevent corporate influence from distorting, delaying, and defeating needed regulation. As the industries profiting from these unhealthy commodities and environments share a playbook of tactics for influencing consumers and undermining public health policies, there is an opportunity for the public health community to apply lessons learned in tobacco control to the prevention of other NCDs (Moodie et al. 2013).
The globalisation of the Tobacco Industry
At the turn of the twentieth century, the tobacco industry reengineered tobacco into the mass-producible modern cigarette (Wipfli and Samet 2016). It also fashioned consumer taste through mass-advertising to create demand for its products (Wipfli and Samet 2016). In the 1950s, scientific advances, led by pioneers such as Richard Doll and Bradford Hill, meant smoking’s harms became ever more apparent and industry had to innovate against the public’s growing awareness to the harms associated with its products and the growing impetus for public health intervention (Wipfli and Samet 2016; US HHS 2014). To do this, it manipulated public opinion and reengineered its products. On the one hand, findings of harm by independent researchers were dismissed through mass-media campaigns while, with the other, novel “light” and “low-tar” filtered cigarettes promising less harm were introduced to ensure continued market growth (US HHS 2014). To bolster both these dismissals and their new so-called healthier products, distorted science was produced and laundered by industry-controlled front-groups furthering the interests of the industry (Wipfli and Samet 2016; Minhas and Bettcher 2010). These efforts to influence individuals and policymakers delayed effective action in high-income countries (HICs) for decades and endured with adaptation as needed through the 1970s, 1980s, 1990s, and continue to this day with newer so-called “reduced risk” and “harm reduction” products of the twenty-first century (Minhas and Bettcher 2010).
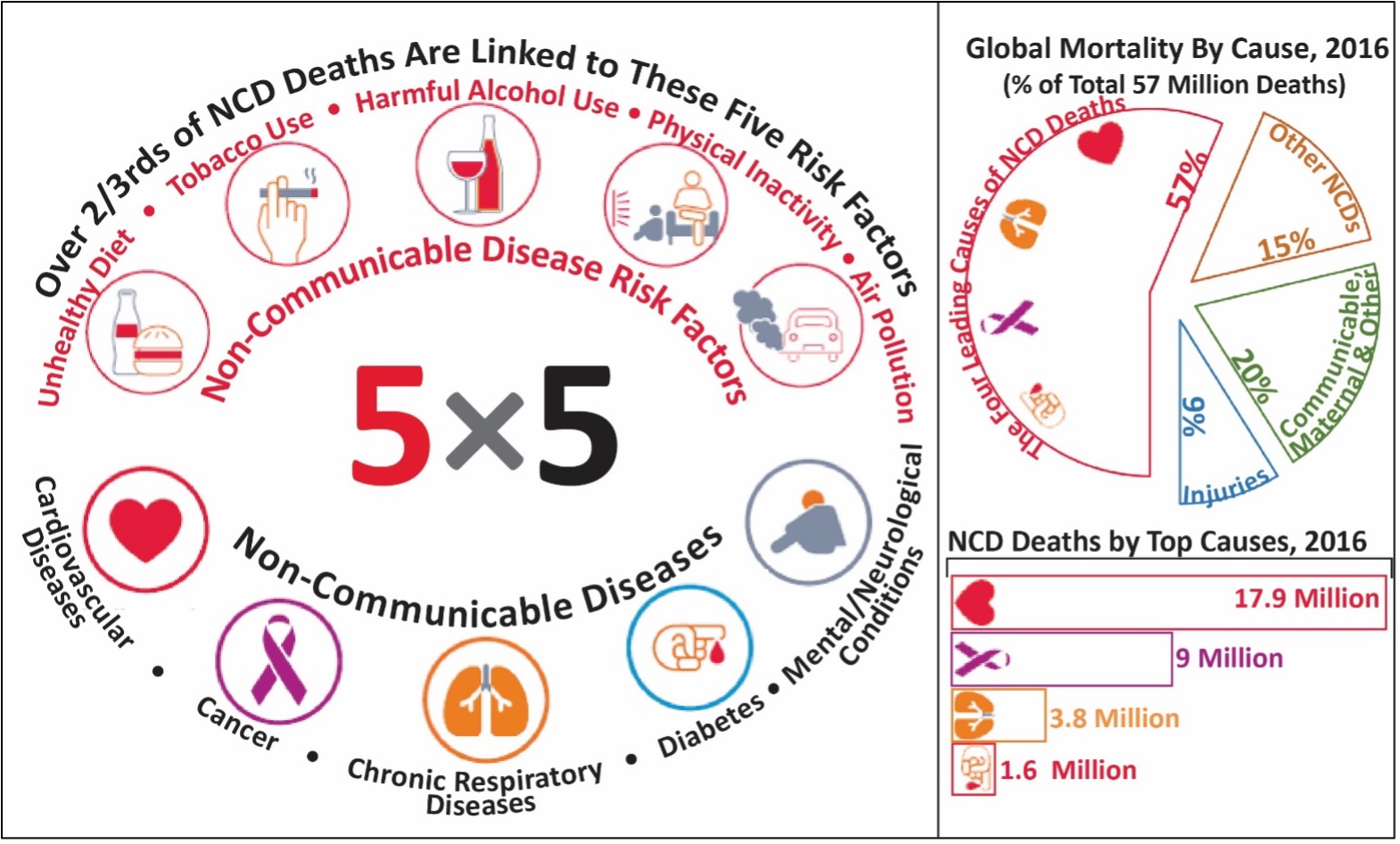
Fig. 1 (Adapted from WHO 2019c; UN Interagency Taskforce 2020)
In the past century, most tobacco-related mortality occurred in HICs but in this century the majority is expected to occur in LMICs. This migration of mortality was precipitated by tobacco’s second wave of globalisation. As regulation improved in HICs from the 1970s onwards, TTCs were forced to seek out new growth markets for their deadly products (Wipfli and Samet 2016; Reubi 2016). Their flight to safer climes was buoyed by the tailwinds of late twentieth-century market liberalisation, which they had a role in encouraging and shaping (Bettcher et al. 2000; Minhas and Bettcher 2010; NCI and WHO 2016). globalisation of trade, investment, and a drive toward privatization meant formerly closed markets were either welcoming of investment or could be legally forced open (Bettcher et al. 2000; Minhas and Bettcher 2010; Gilmore et al. 2015). TTCs have sought to expand consumption in these markets with a familiar, although often even bolder, playbook of influencing individuals and governments to use and permit its products through deceit, obfuscation, and outright illegalities (Bettcher et al. 2000; Gilmore et al. 2015). By the late 1990s, the global market was dominated by one state-owned enterprise and four TTCs (Gilmore et al. 2015; Wipfli and Samet 2016; NCI and WHO 2016). These TTCs became increasingly reliant on sales growth from LMICs where they began to locate most of their manufacturing and where, by 2015, over 90% of tobacco leaf was grown (Gilmore et al. 2015; NCI and WHO 2016). But this shift of production and demand was not accompanied by a migration of high-value work – for example, research and development, marketing – or corporate profit, still largely located in HICs (Wipfli and Samet 2016; NCI and WHO 2016). Accordingly, LMICs were subjected to immediate economic exploitation and an increasing burden of devastatingly expensive tobacco-related disease.
Combating the Tobacco Industry: An Introduction to Tobacco Control and the WHO FCTC
During the early decades of tobacco industry’s globalisation, 1940–1980, response centred on action at national level with global coordination mostly confined to endeavours to build collective knowledge on tobacco control best practice and create momentum for effective tobacco control – as prominently enacted in a series of “World Conferences” on tobacco control, beginning in 1967 with the First World Conference on Tobacco and Health in New York City (Reubi 2016). Beginning in the late 1960s, the first major tobacco control initiatives in HICs, then at the peak of their epidemics, centred on reducing demand for tobacco by warning and educating the public about its harms as well as providing cessation services and advice to assist those seeking to quit (Wipfli and Samet 2016; Reubi 2016; US HHS 2014). Another measure, tobacco taxes, that had long been used only as means for raising revenue came, by the 1980s, to also be seen as a mechanism for increasing price and thereby reducing demand for tobacco (Wipfli and Samet 2016; World Bank 1999; US HHS 2014). With ever more research independent of the tobacco industry, led by figures such as Takeshi Hirayama, tobacco control’s toolbox expanded further in the 1980s as evidence on nicotine’s addictiveness and second-hand smoke’s harms, in particular to children and women, concretised and finally overcame industry obfuscation (Hirayama 1981; Wipfli and Samet 2016; WHO 2010; US HHS 2014). In the decade that followed countries began to restrict smoking in indoor and public places as a means of protecting nonsmokers from harm while also denormalising tobacco use and thereby reducing demand for it (World Bank 1999; US HHS 2014; Wipfli and Samet 2016; WHO 2010; Drope et al. 2018). For an example of this gradual progression in evidence and tobacco control measures, see Fig. 2, below.
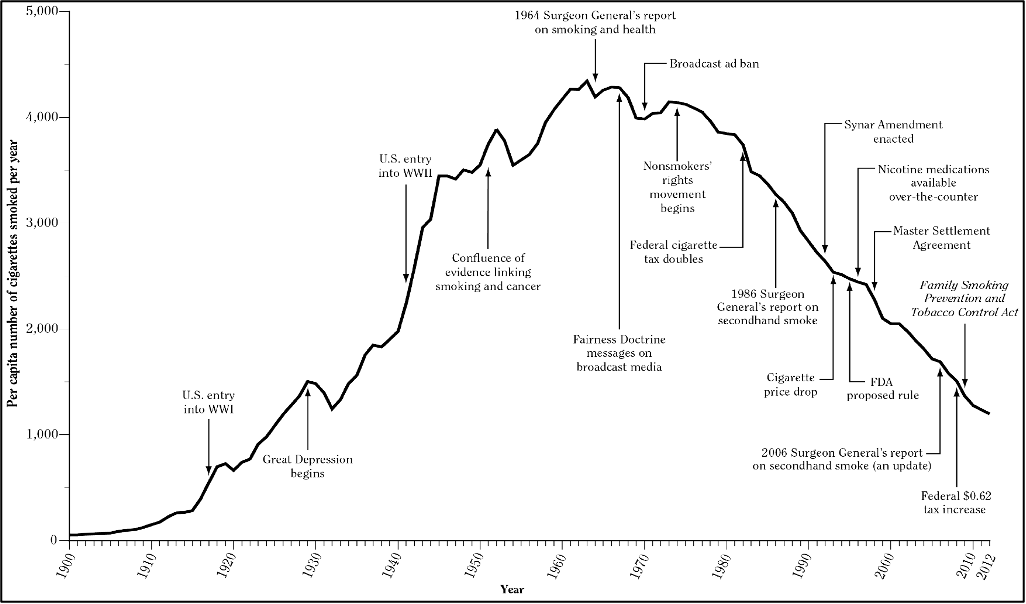
Fig. 2 Adult per capita cigarette consumption and major smoking and health events, United States, 1900–2012 (US Surgeon General 2014)
n response to its increasing penetration of LMICs, in the 1980s and 1990s, international organisations, particularly the World Health Organization (WHO), and civil society stepped to the forefront in a campaign to prevent history’s recurrence – yet another belated response – but with countries that could even less afford this failure (Reubi 2016). With negotiation commencing in 1999, the WHO FCTC was erected on the foundation of evidence on the science of tobacco related disease, national practice in tobacco control, and to combat the interference of industry accumulated over the previous 50 years. This evidence had been won slowly and at the cost of many lives in HICs whose epidemics had, by this time, considerably waned (see Fig. 2, above, for an exemplar, the United States). As well as ensuring momentum for tobacco control continued everywhere, the WHO FCTC aimed to hasten a rapid transference of this tobacco control best practice from HICs to LMICs (Reubi 2016). Fifteen years after its entry into force, in 2005, over 90% of the world’s population is covered by the WHO FCTC and most of the world’s population is covered by at least one highly effective tobacco control measure (WHO 2019a). Although tobacco is still far from elimination and the tobacco industry far from defeated, there is evidence that the tide is turning on the global epidemic: prevalence has been steadily decreasing and the number of tobacco users, which peaked in 2018, is projected to decline in the years to come (WHO 2019b).
In the same way that the tobacco industry acted as a forerunner for strategies that have since been adopted by the food and beverage industry, the WHO FCTC and its implementation is a pathfinder in the struggle to combat the other risk factors for the NCDs pandemic. Market saturation in HICs means these industries have, as with tobacco, needed to penetrate the market of LMICs, which they are becoming increasingly reliant on for growth (Moodie et al. 2013). As with TTC, the food and beverages market control is increasingly consolidated in a handful of global conglomerates (Moodie et al. 2013). As some of these industry actors are deploying similar strategies of influence, deception, and interference used by the TTC, the global health community needs to respond by using the success of the WHO FCTC and its implementation as a pathfinder. With the success of the WHO FCTC, there have been calls to follow its exact formulae by adopting a multilateral treaty binding at international law for other NCD risk factors – in particular alcohol consumption – and corollary maneuvering by the food and beverage industries to head off this possibility (Burci 2018). But its implementation has also been impelled through soft-law (nonbinding) technical guidance, implementation guidelines, and overriding frameworks and this success offers a pathway to progress on other NCD risk factors even in the absence of new multilateral conventions.
Overview of Tobacco-Related Disease and Prevalence
Tobacco Use, Trends, and Disparities
Although global tobacco use prevalence and the overall number of tobacco users has been decreasing for over two decades, the number of male tobacco users only peaked in 2018 and population growth means that overall declines in tobacco user numbers have been gradual – see Figs. 3 and 4, below (WHO 2019b). As seen in Table 1, below, the overall number of users is continuing to grow in the African and Eastern Mediterranean regions and is experiencing only gradual declines in the Western-Pacific and South-East Asian regions (WHO 2019b). Already nearly 80% of smokers are in LMICs and this proportion is only set to increase with future population growth and as certain countries in the early stage of their epidemic see an increase in prevalence (WHO 2019b; NCI and WHO 2016). Of those countries experiencing rises in tobacco use prevalence, three (Congo, Lesotho and Niger) are in the African region and two (Egypt and Oman) are in the East Mediterranean region (WHO 2019b).
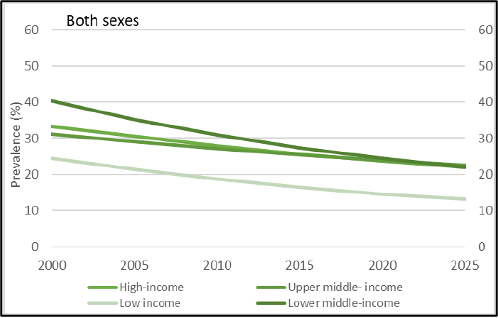
Fig. 3 (WHO 2019b): Trends in global prevalence of tobacco use prevalence among adults by World Bank income group.
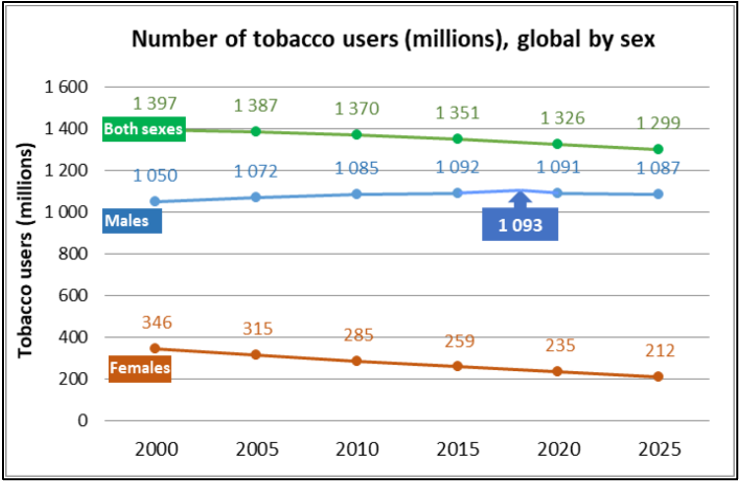
Fig. 4 (WHO 2019c): Trends in the global number of adult tobacco users by sex.
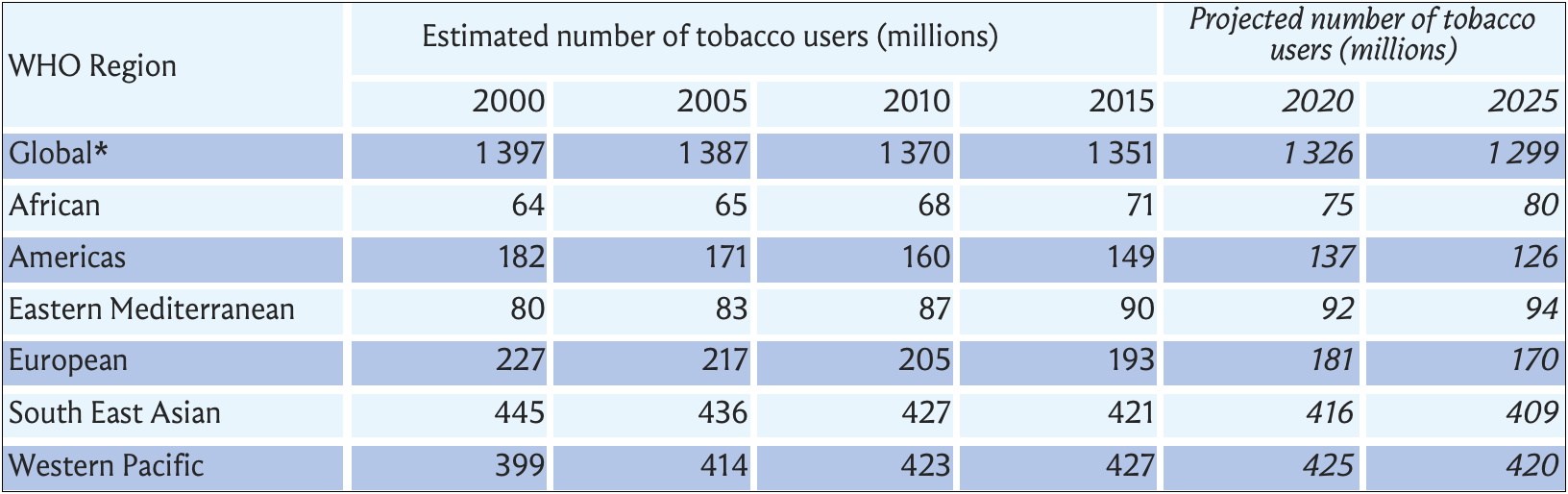
Table 1 (WHO 2019b): Global number of tobacco users.
Within all countries but in particular LMICs, men use tobacco at a much greater rate than women and reduction in their use among men has been relatively difficult to achieve (WHO 2019b). Because of this the voluntary target established at the World Health Assembly (WHA) for a 30% relative reduction in prevalence between 2010 and 2025, for people aged 15 years and over, is not on track to being met with only a 23.4% decline projected (WHO 2019b). Although tobacco use prevalence among women is declining faster than with men, they are a demographic that has been and still are heavily targeted by the tobacco industry as a potential growth market (see Box 2, below). Adolescents are also a demographic of concern for tobacco control proponents and interest from the tobacco industry as those who take up tobacco use at a young age are most likely to become addicted and most tobacco users are ushered into what can be lifelong addictions at a young age (Drope et al. 2018). Globally, 30% of those in the poorest quintile smoke compared to 21% of those in the wealthiest quintile (Marquez and Moreno-Dodson 2017). This divergence between the rates of tobacco use by those who are more affluent and those who are poorer is particularly pronounced in LMICs where prevalence among the bottom quintile can be 1.4 to 1.8 times greater than prevalence among the highest quintile (Marquez and Moreno-Dodson 2017).
Box 2: A Gendered Framework for Understanding Tobacco and Tobacco Control
Over the course of the last century and still in most of the world, a person’s gender is the strongest predictor for tobacco use (WHO 2010). It is also the strongest predictor for exposure to second-hand smoke with more attributable deaths among women than men (573,00 vs 311,000) globally in 2016 (Drope et al. 2018). Tobacco use has been and still often is gendered as male and integrated into aspects of social life in which women have been and still are made marginal (WHO 2010). Over the last four decades, this gender gap has narrowed or disappeared in many HICs as seen in statistics on tobacco use prevalence and tobacco attributable deaths in many HICs – see Fig. 5, below (Jannsen 2019). For example, in Australia, Canada, Denmark, Iceland, Ireland, New Zealand, Norway, Sweden, the United Kingdom, and the United States smoking attributable mortality among women is similar or even higher than among men (Jannsen 2019). As depicted in Fig. 5, below, this is occurring because women typically took to tobacco between one decade to two decades later than men so both their use prevalence and attributable mortality peaked later – with in some cases the latter still having not peaked (Jannsen 2019; Thun and Freedman 2017).
The rise in female tobacco use in HICs over the course of the twentieth century was not, however, a natural phenomenon but rather one driven in large part by tobacco industry machination (WHO 2010). Through innovating tobacco products and marketing techniques the industry managed to access a previously untapped market of women smokers in the 1940 through to the 1960s (WHO 2010). There exists an even larger untapped pool of potential customers in women across many LMICs – this is one of its greatest potential sources of future revenue growth and profit. Already the tobacco industry has succeeded in expanding female consumption in middle-income markets across Latin-America, the former Soviet Union, and parts of Asia through aggressive marketing and price tactics tailored toward women (Gilmore 2012; WHO 2010; Drope et al. 2018). But in LMICs there still remains an opportunity to prevent the tobacco industry from replicating these tactics and obstruct a rise in female tobacco use rates similar to that seen in HICs. This will, however, require policymakers to adopt a gendered lens on tobacco control that recognises both how tobacco industry tactics are tailored according to gender and how public health interventions to prevent use and encourage cessation have to be tailored (WHO 2010, 2019a).
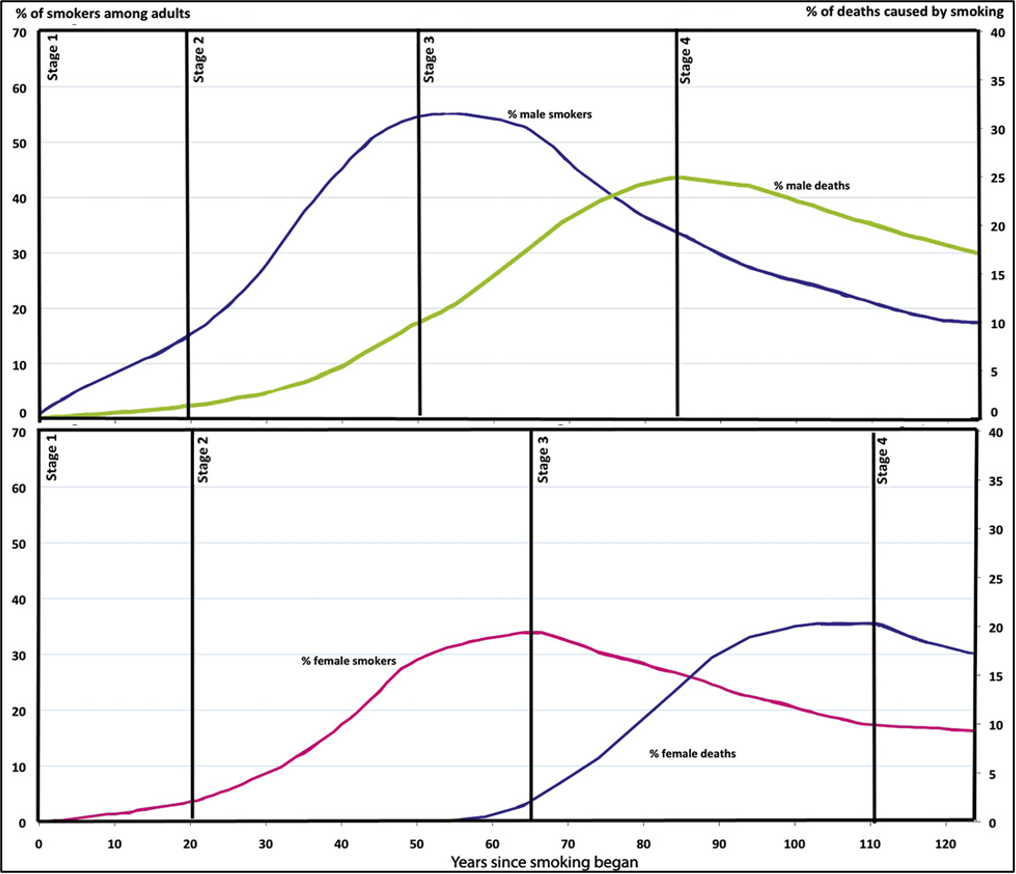
Fig. 5 (Thun, et al, 2012): The gendered stages of the tobacco epidemic in HICs.
Tobacco-related disease
Tobacco, a highly addictive substance, is the only legal product that kills up to half of its consumers when used as intended by its manufacturers: long-term smokers face a threefold higher risk of death and lose, on average, at least a decade of life (NCI and WHO 2015; Marquez and Moreno-Dodson 2017; Drope et al. 2018). Compared with nonsmokers, smokers have twice the risk of stroke, a fourfold risk of heart disease, are over three times more likely to develop chronic obstructive pulmonary disease, 22 times more likely to develop lung cancer, and are exposed to a greater risk of developing a variety of other cancers (US HHS 2014; Drope et al. 2018). This is in addition to various other forms of tobacco-related morbidity and the effects that exposure to tobacco has on foetal development and viability (US HHS 2014; Drope et al. 2018). There are also comorbidities with infectious diseases such as tuberculosis, human papillomavirus, HIV infection, and many infections of the lower respiratory system, including influenza and COVID-19, as well as mental health conditions and substance abuse disorders (US HHS 2014; Thun and Freedman 2017; Drope et al. 2018). Tuberculosis is particularly exacerbated with both its chance of transforming from its latent to active state doubled and its overall progression being worsened by tobacco use (US HHS 2014; Drope et al. 2018). Further, tobacco use is a principal risk factor for many relevant NCDs that are, in turn, major risk factors for those with COVID-19 (Mehra et al. 2020; UN Interagency Taskforce 2020; Kluge et al. 2020). Smoking is also associated with greater disease severity and risk of death from COVID-19 (WHO 2020; Mehra et al. 2020).
The overall burden of tobacco-related disease composes a significant share of NCDs, the largest contributor to global mortality and morbidity, 71% of total annual deaths (WHO 2018b). For smoking alone, there were nearly 150 million attributable DALYs (disability adjusted life years) worldwide in 2015 (GBD 2015 Tobacco Collaborators 2017). This made it the leading risk factor for attributable disease burden in 24 countries and among the top five risk factors in over 109 countries (GBD 2015 Tobacco Collaborators 2017). On present trends, tobacco use is projected to, by 2030, exceed other leading risk factors in producing the greatest burden of mortality and disability globally (NCI and WHO 2016). Because LMICs are currently at the earlier stages of the epidemic and are also experiencing greater relative income growth (see Fig. 5, above), the vast majority of the increase in the burden of tobacco use is expected to occur in LMICs (NCI and WHO 2016; Drope et al. 2018). As many tuberculosis cases are found in LMICs, particularly in South-Asia and sub-Saharan Africa, the comorbidities between tobacco use and tuberculosis makes increases in their tobacco use burden particularly concerning (Drope et al. 2018).
Nicotine and Tobacco Products
There is a plethora of tobacco products available on several markets globally. These products, which can be broadly categorised into: (1) cigarettes; (2) other smoked tobacco products; (3) novel and emerging nicotine and tobacco products; and (4) smokeless tobacco products, have evolved over the years, with the primary purpose of increasing appeal and sustaining use. The content, emissions, and design features of these products contribute to their appeal, influence consumer use, as well as consumer perception of harm. Thus, these three characteristics of nicotine and tobacco products influence their attractiveness, addictiveness, and toxicity which can vary depending on the product in question and contribute to the negative health consequences elicited by the products – see Fig. 6 (WHO 2018a). It is, however, important to keep in mind that these negative consequences go beyond toxicity, which is often equated to and misrepresented as “harm” to an individual (WHO 2018a). “Thus, reduced exposure to toxicants may or may not translate to better health outcomes” (WHO 2018a). A product’s heightened appeal or nicotine content, which drives addictiveness, may offset any potential benefits from reduced exposure of people to toxic compounds over a longer period of time (WHO 2018a). Importantly, “all forms of tobacco products are toxic, encourage and support use and addiction, and have the potential to cause harm” (WHO 2018a).
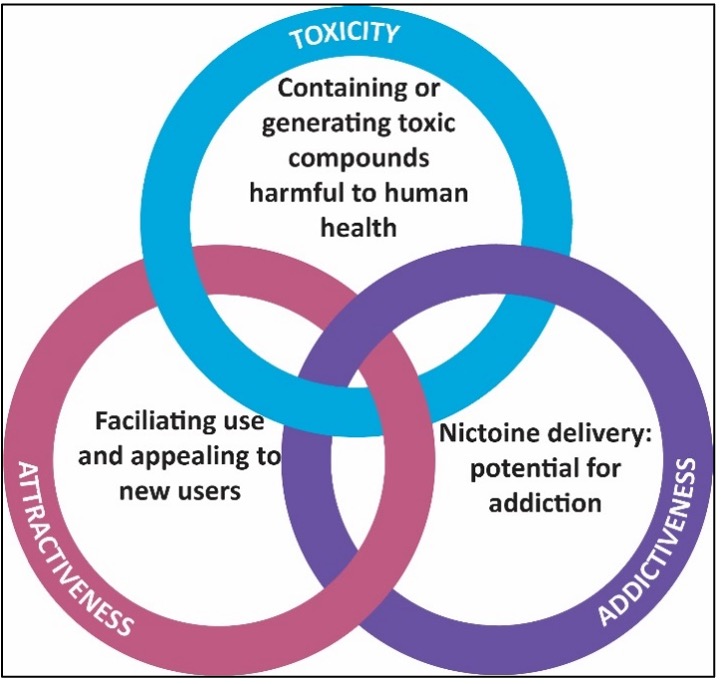
Fig. 6 (Adapted from WHO 2018a): Intertwined factors supporting the negative health consequences of tobacco products.
Of all tobacco products cigarettes are the most common and their use accounts for over 90% of tobacco sales worldwide. They are also the most popular tobacco products in HICs and its manufacture and marketing is concentrated in the four major TTCs based in HICs, as well as China’s state-owned tobacco monopoly (NCI and WHO 2016; WHO 2018a). Other smoked tobacco products include waterpipe tobacco, cigars, bidis (a cheap, hand rolled smoked product common in India and Bangladesh), and kreteks (a clove cigarette common in Indonesia), with some, particularly waterpipe tobacco, now gaining popularity in parts of the world not previously common (NCI and WHO 2016; WHO 2018a). This may be partly due to the belief held by users that some of these products, such as water pipe tobacco are less harmful than cigarettes, despite the accumulating evidence on their harms to human health, which are similar to cigarettes, albeit less-well researched (Thun and Freedman 2017).
Novel and emerging nicotine and tobacco products, which for the purposes of this report, have been classified into three broad categories namely electronic nicotine delivery systems (ENDS), electronic non nicotine delivery systems (ENNDS), and heated tobacco products (HTPs) are discussed in detail in section “Partnerships for Action on Tobacco Control.” But it is worth noting that these products have disrupted the “norm” with respect to tobacco control and thus cannot be ignored in tobacco product regulation. The aggressive marketing of these products, their market positioning and strategic promotion, mainly as “reduced risk” products, despite mounting evidence that some are as harmful as cigarettes, further complicates tobacco control.
In terms of smokeless tobacco, there are over 303 million users around the world compared with 1.1 billion adult smokers (WHO 2019b). A small portion of these people are using a novel form of snuff (ground or powdered tobacco) known as snus – see Box 3, below (WHO 2010). However, most of them use traditional chewed products, such as gutka, which is common in WHO’s South East Asian Region (with at least 248 million users, over 80% of the total) and amounts to 24% of the region’s men and 11.5% of women (WHO 2019b). Notably, smokeless tobacco use is seven times more common than smoking among women in this region (WHO 2019b). Their consumption in this region poses a particular challenge to regulators because there is significant product variation as production is generally less standardised relative to cigarettes with assembly most often occurring locally and by hand (NCI and WHO 2016). Such production practices also exacerbate uncertainty as to their effects on human health (Thun and Freedman 2017). Furthermore, smokeless tobacco products are often believed to be and marketed as safer for consumption than smoked tobacco products but in fact are highly addictive and hazardous (WHO 2019a; Thun and Freedman 2017). It is estimated at least 100,000 global deaths are attributable to smokeless tobacco use annually with causative links established between this use and cancers of the esophagus, oral cavity, and pancreas (Thun and Freedman 2017).
Box 3: Snus
Snus, a smokeless tobacco product and a type of moist snuff, rose to popularity in Sweden and Norway in the 1980s (Evan-Reeves et al. 2020). Although relatively uncommon globally, it is notable for the claims by its proponents that it poses reduced risks for human health relative to conventional tobacco products (NCI and WHO 2016). While these products may reduce toxicity to users at the individual level relative to smoking, they are still toxic and carcinogenic with causative links to cancers of the oral cavity and pancreas (Thun and Freedman 2017). Note also that there is variation in snus product content and design with some being both more toxic and addictive (Thun and Freedman 2017). In addition, because of snus’s attractiveness and promotion as a relatively “less harmful product” that can be used in smokeless spaces and discreetly there are concerns that it may cause harm at the population level (NCI and WHO 2016; Evan-Reeves et al. 2020). There is particular concern, as they may appeal to young people, who have never used tobacco, as well as those who would otherwise have quit entirely (NCI and WHO 2016; Evan-Reeves et al. 2020).
Global Context of the Tobacco Epidemic
The Economic Cost of Tobacco Related Disease
Annual global economic loss attributable to the total tobacco-related disease burden is estimated at US$1.4 trillion which is equivalent to 1.8% of annual global GDP (Goodchild et al. 2017; Marquez and Moreno-Dodson 2017). This figure comprises both direct costs, US$422 billion, in healthcare expenditure and indirect costs, close to a trillion USD, in lost productivity (Goodchild et al. 2017; Marquez and Moreno-Dodson 2017). Of this direct and indirect cost, 40% is incurred by LMICs (Marquez and Moreno-Dodson 2017). In the absence of effective interventions to reduce tobacco demand and assist tobacco cessation, costs to LMICs will escalate as their presently young tobacco users mature into elevated chronic disease and mortality (Marquez and Moreno-Dodson 2017). This dire forecast is not assisted by the fact that the number of tobacco users – and in some cases, prevalence of use – continues to increase in many LMICs (WHO 2019b). In both HICs and LMICs, the inequitable distribution of tobacco use prevalence means widening social and economic disparities as household expenditure is diverted to servicing nicotine addictions. Those least able to afford lost productive years and increased healthcare costs disproportionately suffer these losses and costs (NCI and WHO 2016; WHO 2019b). LMICs are, moreover, less able to absorb the rise in tobacco-related morbidity and associated economic costs than HICs were at the peak of their tobacco-related disease burden. This is due to their urgent need for economic development and their often more fragile health systems and social safety nets, which together leave poorer households particularly threatened (Marquez and Moreno-Dodson 2017; WHO 2019b). Accordingly, the tobacco epidemic is not only a tragedy for life, health, and equity within societies but also threatens global aspirations to universal health coverage, economic security, and sustainable development (WHO 2019b).
The Economics of Consumption
This tragic burden and pattern of tobacco consumption is a product of tobacco industry artifice in both creating, spreading, and sustaining the tobacco epidemic. In pursuit of growth, the tobacco industry has no choice but to maximise consumption of their addictive and dangerous products by penetrating and then expanding into new markets. With the vehicle of investment and trade liberalisation, the TTCs entered and bought up most markets over the 1970s, 1980s, and 1990s and now their growth prospects depend on expanding consumption in these markets (Gilmore et al. 2015). Low prices and aggressive advertising toward key groups, young people, women, and vulnerable populations, are essential for growth in these emerging markets (Gilmore et al. 2015). The foundation of this strategy is the standard playbook of industry interference: to protect the potential for growth in these markets, regulations, particularly taxes, must be preempted, undermined, and evaded (Gilmore et al. 2015; NCI and WHO 2016).
In established markets, TTCs need to increase profits per tobacco user while also minimising reductions in the number of tobacco users. One tactic for extracting profit in the face of declining volume of sales is “overshifting” taxes: increasing price by more than increases in excise tax and then blaming the entire price rise on the tax (Evan Reeves et al. 2020; Gilmore et al. 2015). But to minimise market contraction, cessation of tobacco products must be discouraged and entrants encouraged – with youth uptake particularly necessary for rejuvenating the customer base in the face of ongoing mortality (Gilmore et al. 2015). “Product segmentation” permits both goals: less attractive cheaper brands are maintained at a low price through increases in the price on more heavily marketed and aspirational premier brands which absorb and exceed the cost of rises in excise on all brands (Gilmore et al. 2015). In this way, cheap brands can encourage price-sensitive young people to enter the market and prevent cessation by price-sensitive poorer people otherwise discouraged by increases in price (Gilmore et al. 2015). Both groups can be kept in the market as customers for volume and potential users of premier brands. To ensure the continued availability of this and other strategies to grow profits while preventing market contraction, TTCs need to undermine and interfere with tobacco control policy.
Tobacco Control: What We Know Works to Reduce Tobacco Use
Countries, particularly HICs, have been applying tobacco control interventions for decades or even centuries. In the eighteenth century, Adam Smith, also known as the “Father of Economics” was one of the first proponents of tobacco taxes – albeit more for the purposes of raising revenue than advancing health. In 1999, the World Bank, which had, over the decade, been increasing its work on chronic diseases with a focus on tobacco-related disease published Curbing the Epidemic. This ground-breaking study reviewed the evidence available on key measures that had been developed to combat the impact of the tobacco epidemic.
Tobacco control policy measures and public health interventions either reduce the supply of tobacco products or the demand for tobacco products. The World Bank Report, as well as a plethora of evidence since, shows that many of these measures are effective and demand-reduction measures that are particularly effective to reduce tobacco use. Fiscal measures like increased taxes which decrease the affordability of tobacco products is a good example of a highly effective demand-reduction measure (US HHS 2014; NCI and WHO 2016). Other non-price measures like ensuring people know the harms associated with tobacco through mass media campaigns and health warnings on tobacco packaging; bans on tobacco advertising, promotion, and sponsorship; and restrictions on smoking in public places have all been shown to be highly cost-effective and help to prevent people from taking up tobacco use and/or help to convince tobacco users to quit (US HHS 2014; World Bank 1999). Evidence also shows that those who want to quit have much higher chances of succeeding if crucial cessation services are made available to them such as brief advice provided by healthcare workers, nicotine replacement therapies, and national toll-free quitlines (WHO 2019a; US HHS 2014; World Bank 1999). As set out in Fig. 7, below, demand reduction measures are highly cost-effective because they give a strong return on investment due to their low, high-efficacy, and the benefits proven to accrue from reduced tobacco consumption in reduced healthcare costs and stronger economies (Goodchild et al. 2016; WHO 2017; WHO 2018c). WHO has produced guidance setting out “best buy” and “good buy” tobacco control measures that are highly cost-effective. For every US$1 invested in good buy measures for tobacco control, a country can expect a return of at least US$7.43 by 2030 (WHO 2018c). For more, see Fig. 7, below.
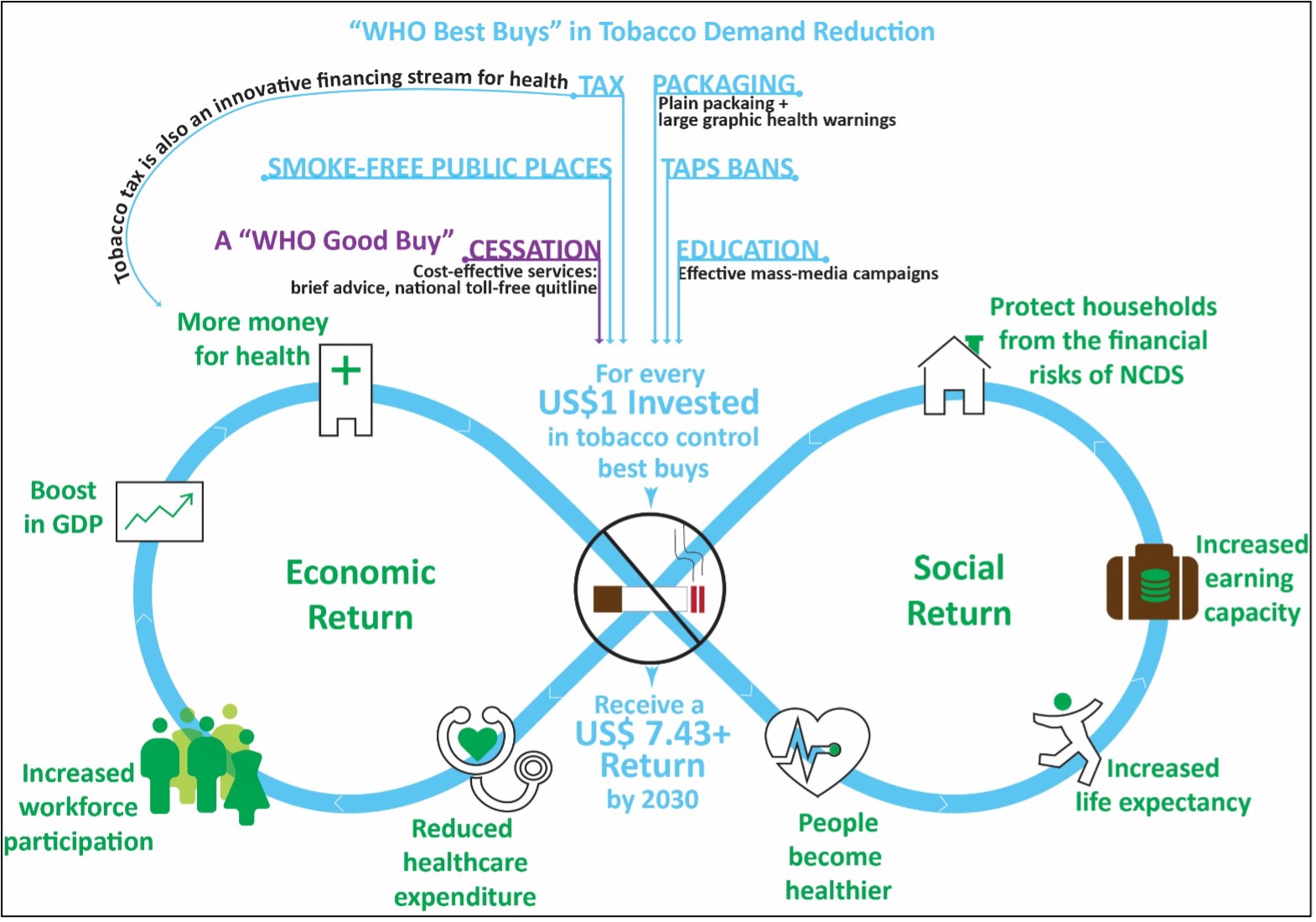
Fig. 7 (Adapted from WHO 2018c): WHO best-buy and good-buy tobacco control interventions.
Other approaches to tobacco control consist of mechanisms to restrict access to tobacco products known as supply-reduction measures (World Bank 1999). These measures include elimination of illicit trade, restrictions on the sale of tobacco products to youth and minors; polices to encourage tobacco farmers to substitute tobacco crops; fiscal measures that provide price-support to tobacco producers to artificially inflate the price of tobacco globally; restriction on international trade; and even full tobacco bans (World Bank 1999). (For more on supply reduction measures see Box 6, below.)
Tobacco Industry Interference
To prevent regulation, the tobacco industry strives to present itself as a stakeholder in economic wellbeing and a responsible partner for government and public health bodies (Bialous 2019; Bialous and Glantz 2018). Although the currency of industry reputability is much debased, this rhetoric is still influential with many governments, although some governments see through the “gimmicks.” Part of its strength lies in presenting tobacco as a driver of economic growth and employment, as a ready source of revenue or investment (Gilmore et al. 2015). This myth is the foundation for a false dichotomy between economic well-being and public health that seeks to reframe the question of tobacco as principally an issue of economy rather than health (Gilmore et al. 2015). This “choice” is put to countries persuasively by industry front-groups, such as the International Tobacco Growers Association (ITGA), and proxies – the US Chamber of Commerce or the International Tax and Investment Centre (Gilmore et al. 2015).
The reality, of course, is that health and economy are inseparable. This is particularly so with tobacco. As noted above, the burden of tobacco-related disease is crushingly large. As elaborated on in Box 5, below, the tobacco industry rhetorically minimises the harm of its products but also overstates the importance of tobacco to the economy and the effect that tobacco control would have on economic well-being (Gilmore et al. 2015; NCI and WHO 2016). Despite dire tobacco industry projections, evidence shows that countries should not experience net job losses – in fact, many studies even show net increases – from even very strong tobacco control efforts, which in reality are also usually incremental in implementation and gradual in effect, permitting ample time for adjustment (NCI and WHO 2016). In the broader economy, expenditure by quitting tobacco users is shifted elsewhere for the generation of equivalent employment and income (NCI and WHO 2016).
Box 4: Economics of Tobacco Farming
LMICs account for the vast majority of tobacco farming – over 90% by either volume produced, or land cultivated – and among these a few select countries are gaining an ever-increasing share of the export market (NCI and WHO 2016; Marquez and Moreno-Dodson 2017). Tobacco is a superficially attractive cash crop which comes with support from deep-pocketed TTCs able to provide loans, equipment, and advanced logistics often lacking for other crops (NCI and WHO 2016). But it comes with strings: hazards to health, environmental degradation, child labour, and an oligopolistic global market dominated by a handful of multinationals with control over prices (NCI and WHO 2016). Because tobacco leaf markets are uncompetitive, industry controls prices and can lock farmers in cycles of debt and poverty (Gilmore et al. 2015; NCI and WHO 2016; Marquez and Moreno-Dodson 2017). Tobacco farming is harmful to human health through green tobacco sickness and heavy pesticide exposure while also being harmful to the environment through soil depletion and deforestation (NCI and WHO 2016). In farming, too, employment has been diminishing with increasing efficiencies in production, and tobacco control programs locally implemented will not affect export-oriented farming (Marquez and Moreno-Dodson 2017). Export-oriented farming depends on global demands, not on local consumption (Marquez and Moreno-Dodson 2017). In the few countries in which production overwhelmingly serves domestic consumption, change will only be gradually and predictably affected by tobacco control programs at home and the political choice is available to help these farmers to alternative crops that can provide a sustainable livelihood (Marquez and Moreno-Dodson 2017; NCI and WHO 2016; Gilmore et al. 2015).
Industry also seeks to portray an image of itself as a partner to government and public health bodies through, for example, its “actions” on illicit trade, its various acts of corporate social responsibility (CSR), and its devotion to “sensible” regulation. Despite an historic record of profiteering from illicit trade and evidence of ongoing complicity in it, through overwhelming expenditure and their unique knowledge of tobacco supply chains, TTCs have managed to project an image of themselves as victims, an authoritative source, and a helping hand (Gilmore et al. 2015). They have then used this position to create partnerships with governmental bodies, including customs or trade officials and try to leverage these into relationships of cooperation with policymakers (Gilmore et al. 2015). CSR plays a similar role, particularly among some LMICs in which tobacco largesse is more needed, helping industry to get closer to the table of decision-making (Gilmore et al. 2015). Finally, TTCs are increasingly adopting the veneer of respectability and atonement in a play for rehabilitation (WHO 2019a; Bialous and Glantz 2018; Evan-Reeves et al. 2020). This can take the form of encouraging weak regulations as sensible compromises to preemptively deflate political impetus for effective tobacco control (Minhas and Bettcher 2010; Gilmore et al. 2015; Bialous and Glantz 2018). In service of this purpose, in particular within HICs, the rhetoric of harm reduction is being repurposed from earlier decades for industry’s novel and emerging nicotine and tobacco products (Bialous 2019).
These efforts to infiltrate and interfere with policymaking are supported by misrepresentation of the science of tobacco products and tobacco-related disease (Minhas and Bettcher 2010; Bialous and Glantz 2018). This began, of course, with brazen dismissals of scientific research into the harms of smoking in the 1950s and the harms of second-hand-smoke in the 1970s (Bialous and Glantz 2018; Evan-Reeves et al. 2020). More subtle was the scandalous innovation of “reduced harm” products such as “healthier” filter-tipped cigarettes and then the “reduced harm,” and ventilated-filter “light” and “low-tar” cigarettes (Minhas and Bettcher 2010; NCI and WHO 2016; Bialous and Glantz 2018; Bialous 2019; Evan-Reeves et al. 2020). Not only were assertions of reduced effect on health packaged into quantifiable “science” by industry front-groups, but their work was then laundered into reputable seeming science through knowingly flawed measuring processes and captive international standard setting organisations (NCI and WHO 2016; Minhas and Bettcher 2010). These products, it turned out, not only deceived consumers into believing their health claims – with many smokers today still believing light cigarettes are healthier – but were found not to be less harmful than usual cigarettes (NCI and WHO 2016; Evan-Reeves et al. 2020). The continuation of this tactic is seen in the branded “harm reduction” novel and emerging nicotine and tobacco devices now being produced by each of the TTCs (see section “Partnerships for Action on Tobacco Control”, below).
Political intimidation and obstruction are industry’s final line of defense against tobacco control policies. In many countries, the predominance of tobacco industry over the commercial determinants of health reflects the imbalance of power and resources between TTCs responsible only for private profit and governments responsible for public health (Gilmore et al. 2015). Because of their massive annual profits, US$50 billion in 2012, and even larger total revenue, which both dwarf the GDP of many countries, industry can charm, threaten, and bribe policymakers (Marquez and Moreno-Dodson 2017; Gilmore et al. 2015; Drope et al. 2018; Vital Strategies 2019). Within the last two decades, there have been numerous instances of exposed bribery by the major TTCs in LMICs and doubtless many more never unearthed (Minhas and Bettcher 2010; Bialous 2019; Drope et al. 2018; Vital Strategies 2019). In many countries with less enforcement capacity, industry can simply ignore government regulations or otherwise subvert them through the use of proxies (Minhas and Bettcher 2010; Drope et al. 2018).
A more legitimate but no less coercive example of the same phenomena can be seen in the use of law by industry. The threat of legal challenges in domestic and/or international forums is able to chill the best regulatory intentions of governments of lower-income and smaller countries – not necessarily on the basis of the legal merits of an industry position but rather because of the time, cost, and resources required to defend public health measures from legal challenges, particularly in proceedings before international tribunals or dispute settlement bodies. There are documented cases of countries delaying or putting aside tobacco control measures because of the fear of a legal challenge (Crosbie and Glantz 2014; Gilmore et al. 2015). There are also documented instances in which industry has disseminated tendentious legal posturing contrary to advice of counsel to discourage governments from implementing effective tobacco control measures (Crosbie and Glantz 2014). The exact number of times legal threats have been offered quietly and regulatory measures delayed or shelved outside of the public gaze is beyond speculation but is likely significant (Gilmore et al. 2015).
Tobacco Control and the Global Regulatory Environment
Origins of the WHO FCTC
Before the WHO Framework Convention on Tobacco Control (FCTC), international action on tobacco control had already begun. The first resolution requesting WHO action on tobacco control was issued by the World Health Assembly (WHA) in 1971. However, it was in the 1980s that a significant turning point occurred when the WHA issued three resolutions expressing concern about the shifting tobacco epidemic towards lower- and middle-income countries (LMICs), and the annual “World No Tobacco Day” was established. During this decade, the WHO Regions also became increasingly involved in tobacco control work, and the “Tobacco or Health” program was established at WHO headquarters. In 1990, it was succeeded by the “Tobacco and Health Unit,” accompanied by an increase in the number of technical support staff in the six WHO Regions. Concurrently, the tobacco industry was actively engaged in preventing increased WHO involvement in tobacco control, particularly in product regulation, by using its proxies (representatives) to influence the process.
Box 5: WHO’s Governance, Headquarters, Regions, and Country Offices
WHO is constituted by the World Health Assembly (WHA), the Executive Board (EB), and the WHO Secretariat (Kelley Lee 2008). The WHA comprises all 194 Member States of the WHO meeting annually to determine and oversee the work of the organisation, through five-year programs of work, and the election of its Director-General, who serves for five-year terms (Kelley Lee 2008). It also may create regulations legally binding on all its Member States, negotiate conventions legally binding on States that ratify them and adopt nonbinding official recommendations (Kelley Lee 2008). The EB, which meets twice a year and is constituted by members elected by the WHA, prepares the WHA’s agenda and also may adopt urgently needed intersessional measures (Kelley Lee 2008). Finally, the WHO Secretariat, which is led by the Director-General, performs administrative, technical, and operational matters assigned to it by the WHA through its headquarters, six regional offices, and 147 country offices, in addition to two field offices – see Fig. 8, below (Kelley Lee 2008; WHO 2019f).
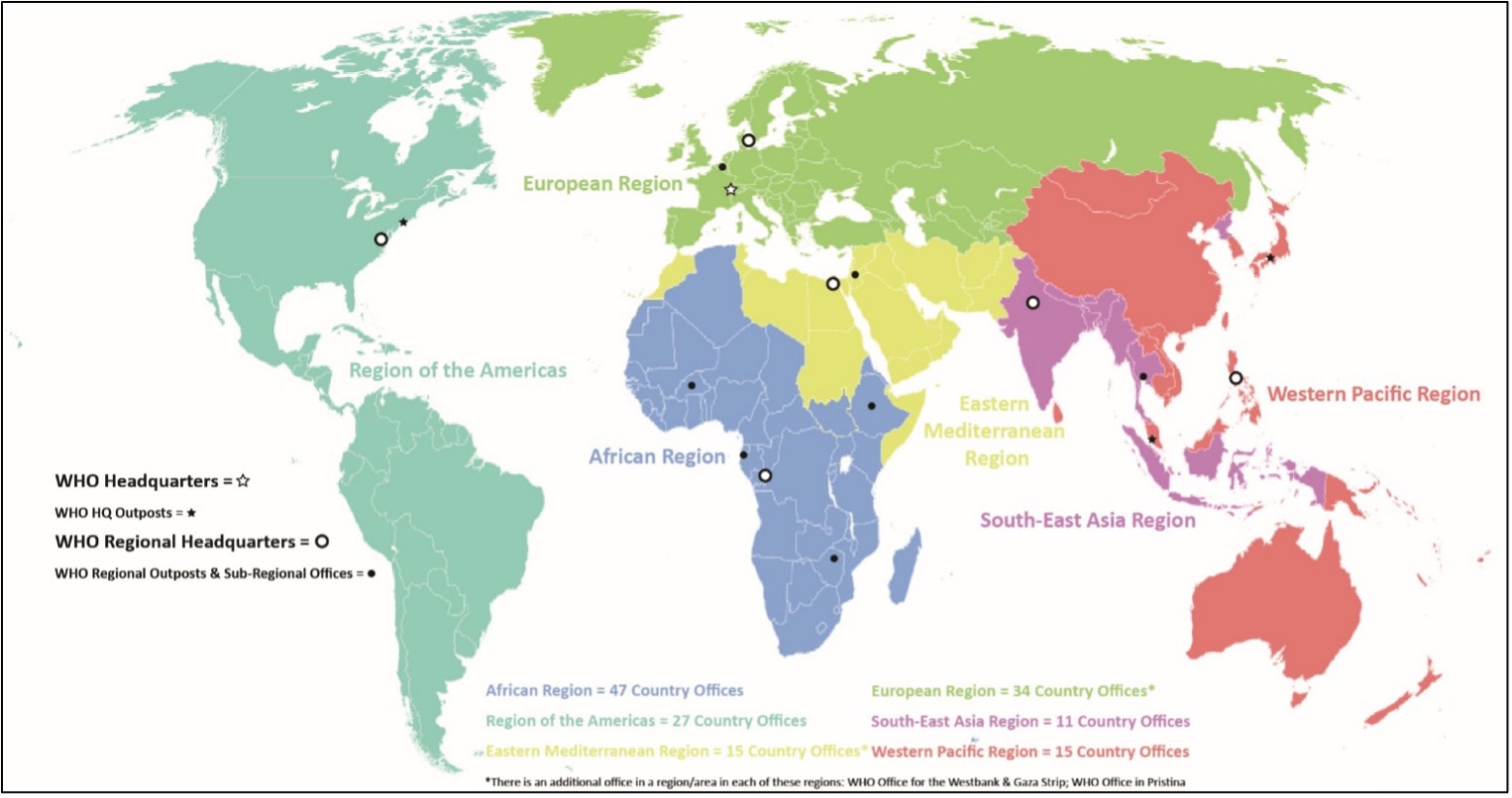
Fig. 8 (Adapted from WHO 2019f): WHO HQ, HQ outposts, regions, regional headquarters, and subregional outposts and offices.
Before the WHO FCTC, there was action at the international level on tobacco control – the first WHA (see Box 5, below, for information on the WHA and the WHO’s governance) resolution requesting WHO action on tobacco control was issued in 1971. But the 1980s marked a turning point as the WHA issued three resolutions expressing concern for how the epicentre of the tobacco epidemic was shifting to LMICs and the annual “World No Tobacco Day” was established (Zhou and Liberman 2018). In that decade, also, the WHO Regions (see Box 5, below) became increasingly involved with tobacco control work and the “Tobacco or Health” program was established at WHO HQ before being succeeded, in 1990, by the “Tobacco and Health Unit” and an accompanying increase in the number of technical support staff in the six WHO Regions (Reubi 2016; Welcome Trust). At the same time, the tobacco industry was engaged in preventing increased WHO involvement in tobacco control, particularly in product regulation, through its proxies (Reynolds and Tansey 2010; Minhas and Bettcher 2010; Bialous and Yach 2001).
Against this backdrop, in 1993, two academics, Ruth Roemer and Allyn Taylor, together devised and subsequently promoted the idea of developing a specific regulatory mechanism for tobacco control (Roemer et al. 2005; Reynolds and Tansey 2010). Then, in 1994, at the Ninth World Conference on Tobacco or Health, Paris, WHO was called on to advance a convention on tobacco control pursuant to a resolution authored by Roemer and Dr. Judith Mackay – a consultant at WHO – and promoted by Taylor (Roemer et al. 2005; Reynolds and Tansey 2010; Wipfli and Samet 2016). This initiated official efforts within WHO to forward development on a treaty and also prompted Canadian engagement with the idea (Wipfli and Samet 2016). Then, in 1995, the WHO’s Executive Board (see Box 5, below), at the submission of the Canadian delegation, instructed WHO’s Secretariat to investigate the feasibility of a declaration or legal instrument for tobacco control (Roemer et al. 2005). Subsequently, in 1996, the WHA adopted a resolution calling for the development of an “international framework convention on tobacco control” (Roemer et al. 2005). Despite the significant agitation in favour of the Convention and earlier activity in tobacco control surveillance and implementation, there were still significant gaps in global data on trends in tobacco use prevalence and the state of tobacco control measures. This was a vacuum which the tobacco industry could fill with their own set of “facts” (Wipfli and Samet 2016).
Preliminary to the real work of drafting and negotiating the text that became the WHO FCTC, a foundation of fact had to be established. Timely contributions were the documents on the secretive practices of manipulation, interference, and outright illegality perpetrated by TTCs that began to be released from 1995 as a result of court settlements and lawsuits in the United States in what would eventually be over 35 million pages of documents (Bettcher et al. 2015). To go further, in 1998, Gro Harlem Brundtland, who had recently became WHO Director-General and, at the urging of Dr. Mackay and Sir Richard Peto, decided to make tobacco control a defining initiative of her tenure, established a WHO cabinet-level project, the Tobacco Free Initiative (TFI), with accompanying increases in budget and a strengthened WHO Regional presence, to help marshal evidence in support of negotiations of the WHO FCTC and coordinate preliminary tobacco control work, particularly in product regulation (Bettcher et al. 2015; Reynolds and Tansey 2010). The World Bank’s ground-breaking report, Curbing the Epidemic, was also published at this time and included evidence that supported many of the measures included in the WHO FCTC (Marquez and Moreno-Dodson 2017).
With the way cleared, work on the WHO FCTC began in earnest in 1999 with the WHA’s establishment of a technical working group to prepare draft elements for inclusion in the treaty, which were completed by May 2000, and the Intergovernmental Negotiating Body that took up the working group’s draft as the basis of negotiations that lasted for three years, concluding May 2003. These negotiations were, however, complex. Many countries had powerful tobacco lobbies pressing them for access and support, and industry used misdirection (the infamous project Cerberus – a de-fanged nonbinding tobacco industry alternative to the WHO FCTC), bribery, and coercion to undermine the negotiations (Bialous and Glantz 2018; Mamudu et al. 2008). As a prophylaxis to backroom deals, WHO ensured the interests of all parties would be open from an early stage by organising, in October 2000, two days of public hearings in Geneva with both public health oriented civil society organisations (CSO) and tobacco industry participation through prior submission and testimony (Mamudu and Glantz 2009). This had the effect of galvanizing and unifying CSOs while also forcing tobacco industry to defend their egregious conduct under the glare of the public eye (Mamudu and Glantz 2009). As a result, CSO activity – already the Convention proposal’s source – proved a counterweight to industry pressure in Geneva and within many countries throughout the negotiations (Bettcher et al. 2015; Reynolds and Tansey 2010).
The WHO FCTC Explained
The result of these negotiations, the WHO FCTC, is one of the most rapidly and widely ratified treaties in the UN’s history and the first convention negotiated by WHO under the power granted it in Article 19 of its Constitution (WHO 2019a). It reached the 40 ratifications required 18 months after its signing and entered into force three months later for less than two years between conclusion and entry into force. Now, with 182 parties, its provisions cover 90% of the global population (WHO 2019a). The Convention specifically frames its provisions to address the “globalisation of the tobacco epidemic” with attention to consequences this has for health, equity, and economy in all countries but particularly LMICs. Its text explicitly modeled on the environmental framework convention approach also evokes the human rights treaties of the UN system and the rights affirmation of the WHO’s Constitution.
Every provision of the WHO FCTC is a legally binding obligation on the States party to it and, as no reservations are permitted, there is no picking and choosing from among them. That said, States Parties are at liberties to determine their own priorities and pace in implementing the majority of the WHO FCTC’s provisions with the exceptions of Articles 11 and 13 which each required a certain minimum level of implementation within, respectively, three and five years of the treaty’s entry into force. Although these measures are listed separately, they are all most effective when implemented together as a package (Bettcher et al. 2015). As set out in Fig. 9, its text comprises three broad categories of obligations as well as other miscellaneous provisions: (1) demand reduction measures at part 3; (2) supply reduction measures at part 4; (3) general obligations at Article 5. Demand measures have proven the most significant for reducing tobacco consumption, but supply measures and Article 5’s provisions are crucial ancillary obligations. Supply measures are discussed in Box 6, below.
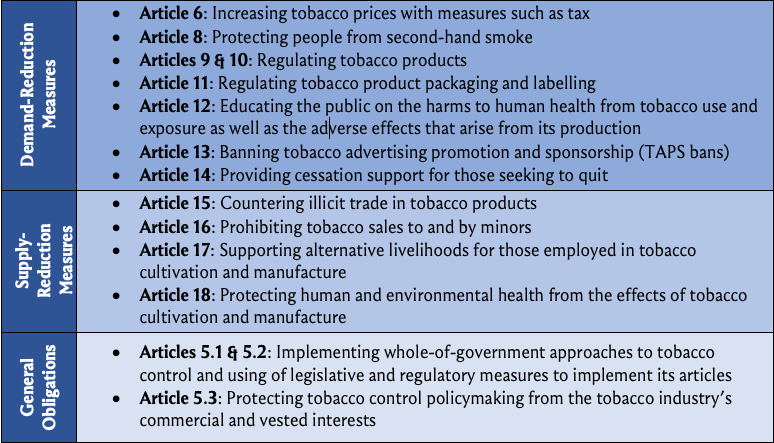
Fig. 9: Key provisions of the WHO FCTC.
Box 6: Supply Reduction Measures and Illicit Trade
Measures to reduce the supply of tobacco products have long been considered less effective at reducing demand but essential to support the evolution toward tobacco’s elimination (World Bank 1999). For example, Article 17, which concerns support for workers transitioning away from tobacco growing and manufacture, is a significant concern in countries that are dependent on tobacco growing for export and employment and an important part of the global compact that the WHO FCTC represents, but is not expected to reduce overall tobacco consumption (World Bank 1999). The need to combat and prevent illicit trade in tobacco products is, however, a key exception to this general rule (World Bank 1999). This is because smuggled products evade national excise, import, and sales taxes and may not conform to nationally mandated warning label and display requirements. In this way, illicit trade undermines efforts to reduce demand by raising prices as well as provide warnings and prevent advertising on tobacco packaging. Despite tobacco industry assertions to the contrary, illicit trade is associated with the effectiveness of customs enforcement, rather than the price of tobacco products, and is best combated through strengthening of these measures, rather than through price decreases (World Bank 1999; Gilmore et al. 2015). As noted in the section “Overview of Tobacco-Related Disease and Prevalence” above, the tobacco industry is a beneficiary rather than a victim of illicit trade (World Bank 1999; Gilmore et al. 2015). As it benefits from and has in the past been exposed as complicit in illicit trade, the industry is part of the problem and will never be a stakeholder in its solution (World Bank 1999; Gilmore et al. 2015).
Demand-reduction measures are divided between price measures, at Article 6, non-price measures, Articles 8–13, and finally cessation support, Article 14. Tax, a price measure, is the single most effective intervention for tobacco control and it is appropriately addressed first (NCI and WHO 2016). Price measures other than tax are not explicitly listed but include interventions, such as minimum price floors and prohibitions on discounting (WHO FCTC COP 2014). Non-price measures are diverse, including obligations to ban tobacco advertising, promotion and sponsorships (TAPS), prevent second-hand-smoke (SHS) exposure with smoke free laws, require product regulation and disclosure provisions, and warn the public of tobacco’s harms.
Under the general obligations, Article 5.3 is often accorded the most importance, although Articles 5.1 and 5.2 mandating a whole of government approach to tobacco control are significant. It requires States to protect their tobacco control policymaking from tobacco industry interference to the extent permissible under national law (WHO FCTC COP 2007). This is a recognition of what has been deemed the fundamental and irreconcilable conflict between tobacco industry interests and the public interest (WHO FCTC COP 2007). This unprecedented attempt to banish the tobacco industry from contributing to policymaking is a clear expression of the disdain felt for their actions. Article 5.3 was, after all, negotiated against the backdrop of the disclosure of millions of formerly private industry documents attesting to the lengths, even into wilful criminality, that TTCs would go to protect and expand the market for their lethal products (Minhas and Bettcher 2010).
The WHO FCTC also contributed to the institutionalisation of tobacco control. This process had begun with WHO’s creation of TFI but was extended with the WHO FCTC’s establishment of a Conference of Parties (COP) and a permanent Secretariat to the WHO FCTC (the Convention Secretariat) that is hosted in, yet legally divisible from, WHO (Bettcher et al. 2015). A protocol to the WHO FCTC, the Illicit Trade Protocol, was adopted by the COP in 2012, and is a related yet separated legally binding treaty with 61 States Parties of its own. Entering into force in 2018, it expands on the WHO FCTC’s illicit trade supply-reduction measures (Article 15) with supply chain controls – a key aspect of which is a global track-and-trace system that is legally required to be established by 2023 – the creation of criminal offences for involvement with illicit trade, cooperation requirements, and due-diligence obligations (Bettcher et al. 2015). While the WHO FCTC’s Convention Secretariat is also the Secretariat to the Protocol, it has its own governance body, the Meeting of Parties (MOP). See Box 7, below, for an overview of the COP and MOP.
Box 7: The WHO FCTC’s Governance Bodies
The COP, which meets once every two years, has two significant normative functions: negotiating protocols to the WHO FCTC and adopting implementation guidelines for the WHO FCTC’s articles (Zhou and Liberman 2018). The latter, guidelines, are important tools that have been deemed subsequent agreement of the parties to the WHO FCTC under the Vienna Law Convention by domestic and international tribunals as well as the International Law Commission (Zhou and Liberman 2018). This means the guidelines are of significant value in interpreting the WHO FCTC’s provisions. Protocols are, like the WHO FCTC, treaties binding on States that ratify them – as of 2020 only a single protocol had been negotiated. The Illicit Trade Protocol’s MOP meets once every two years and does so back to back with the COP (Bettcher et al. 2015). Article 33 of the Protocol provides that, at sessions of the MOP, its States Parties are to provide guidance on implementation, assess progress implementation, and elaborate on certain provisions such as through negotiation of a global track and trace regime.
A key role for the Convention Secretariat is supporting the meetings of the COP and MOP, as well as any subsidiary bodies they establish (Zhou and Liberman 2018). In addition, however, the Secretariat tracks and advances implementation of the WHO FCTC and the Illicit Trade Protocol. It advances implementation through policy support to all countries – but in particular to LMICs, as seen in its FCTC 2030 project – and its establishment of partnerships for tobacco control, see more on this in section “Tobacco Control Implementation” (Zhou and Liberman 2018; WHO 2019a). WHO complements the Convention Secretariat’s policy support by providing States Parties with technical support in their implementation of the WHO FCTC and its Protocol’s key measures and reporting requirements through its six regional offices, headquarters, and 147 country offices (WHO 2019f). These country offices were and continue to be instrumental in encouraging and assisting ratification of both the Convention and its Protocol by the WHO Member States in which they are present (WHO 2019f).
Tobacco Control’s Broader Regulatory Context: Action on NCDs at the United Nations
The tobacco epidemic occurred within a normative void on NCDs and an overwhelming focus on communicable diseases within international health work. This changed with the WHO FCTC’s adoption in 2003, and, since that landmark achievement, there has been substantial progress in building up a framework for combatting all the causes of NCDs, including tobacco, in an integrated fashion. The most comprehensive component of this framework is the UN’s 2030 Agenda for Sustainable Development and its high-profile Sustainable Development Goals (SDGs). The 17 SDGs – see Fig. 10, below – are complemented by 169 targets and various indicators that together compose an indivisible package for economic and social transformation that has significant ramifications for manifold determinants of human health. In a break from the paradigm of the prior Millennium Development Goals, the SDGs bring equity and all aspects of health, including NCDs and tobacco control, directly into the picture, and applied to all countries, HICs and LMICs, on a basis of universality. Its recognition of health’s indivisibility from each of its aspects and from sustainable development is proven prescient with the COVID-19 pandemic. Exposure to tobacco, including through second-hand smoke, caused 100 million deaths in the twentieth century. It is now the cause of eight million deaths annually and is projected to cause one billion deaths in the twenty-first century (NCI and WHO 2016; WHO 2019a).
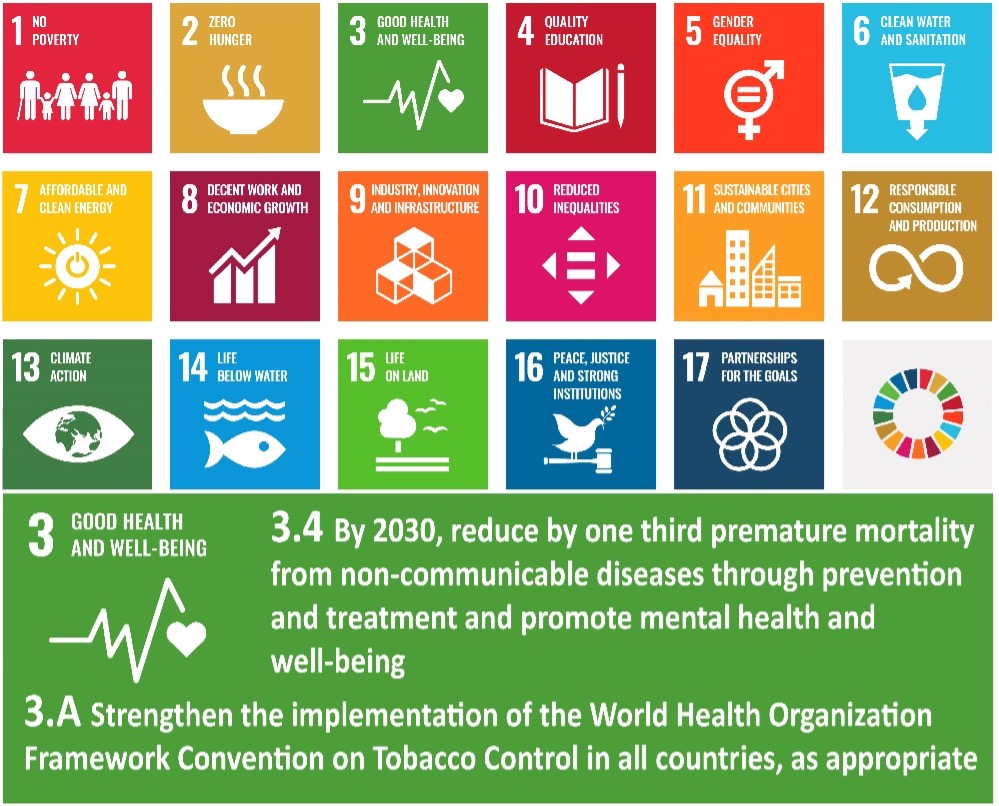
Fig. 10: The sustainable development goals and selected targets under goal three.
Although many of the other goals underpin crucial determinants of health, SDG 3 makes an explicit commitment to ensuring health and well-being for all and was a recognition of how human health is critical to economic development and equity. It established ambitious targets on maternal and child health, communicable diseases, and NCDs. Although there have been successes and some countries are on track, projections suggest that substantial acceleration in progress on nearly all these targets is needed for there to be a prospect of their achievement (WHO 2019c, b). For example, target 3.4, which relates to NCDs, is projected to see real progress but without substantial acceleration in current efforts, it will not be realised – see Fig. 11, below (WHO 2019c). The achievement of the SDGs is made even more challenging by the COVID-19 pandemic and the accompanying global economic recession, but action on target 3.4 through tax measures is a promising solution for raising immediate revenue for strained healthcare systems while also saving lives and preventing mid-term fiscal burdens (Marquez and Moreno-Dodson 2017; Zhou and Liberman 2018; WHO 2019c).
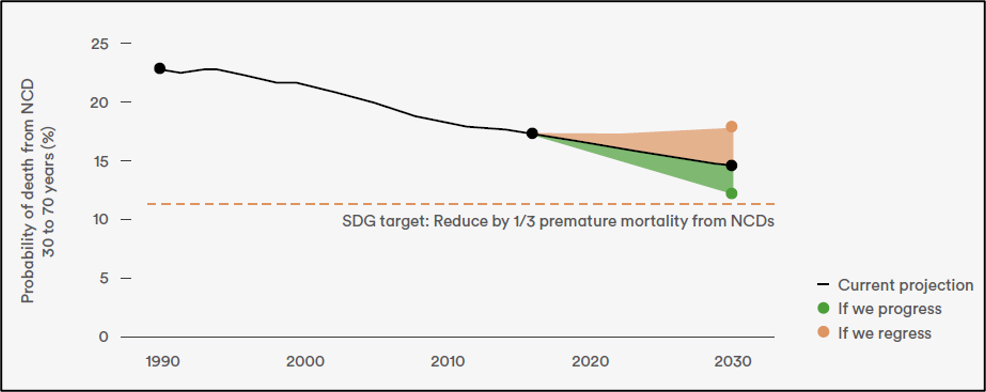
Fig. 11 (WHO 2019c): Progress on SDG target 3.4: global probability of death from NCD between ages 30 and 70.
At the 2011 UN High-Level Meetings on the prevention and control of NCDs, the world committed to a reduction in mortality from four leading NCDs (WHO 2019c). Subsequently, the WHA adopted a set of NCD and risk factors targets, including a 25% relative reduction in premature mortality (ages 30–70 from the four leading NCDs). In the context of this increasing prominence on the international agenda, SDG 3.4 elevated action on NCDs with recognition of substantial progress on their prevention and treatment as essential to development and social equity. The specific aim under SDG 3.4 is reduction by one-third of premature NCD mortality with a focus on the leading NCDs (cancer, cardiovascular disease, chronic respiratory disease, and diabetes). Key to this goal’s achievement are the commercial determinants of health, in particular tobacco use (WHO 2019c). Uniquely, the WHO FCTC is specifically cited with target 3.A calling for all countries to strengthen the Convention’s implementation. Although other legal instruments are implicitly evoked by and interlinked with the goals, the WHO FCTC is the only international treaty specifically referenced, let alone made its own target, in the SDGs and its inclusion reflected the growing priority of tobacco control in the international agenda. Target 3.A is to be achieved by reductions in tobacco use prevalence. Similarly, target 3.5 calls for reducing per-capita alcohol consumption by volume.
Tobacco Control’s Broader Regulatory Context: WHO’s 2019–2023 Programme of Work
Within WHO’s 13th, and latest, programme of work (GPW13), see Fig. 12, below, the WHO FCTC’s influence. It features as an exemplar of how WHO’s normative work can lead to healthier lives with buy-in from Member States, targeted implementation guidance from WHO, and engagement from civil society (WHO 2019d). The GPW13 tobacco control agenda, which is oriented toward the Convention, is also a key component of the target of one billion more people living healthier lives which, among other things, promotes action on the determinants of health and reductions in risk factors to produce healthier environments that foster fewer premature deaths (WHO 2019d). Ensuring these one-billion healthier lives through action on tobacco control and the broader NCD Agenda, as outlined in WHO’s Global Action Plan NCDs, is a way for WHO to advance the achievement of multiple SDG targets in a coordinated fashion (WHO 2019d).
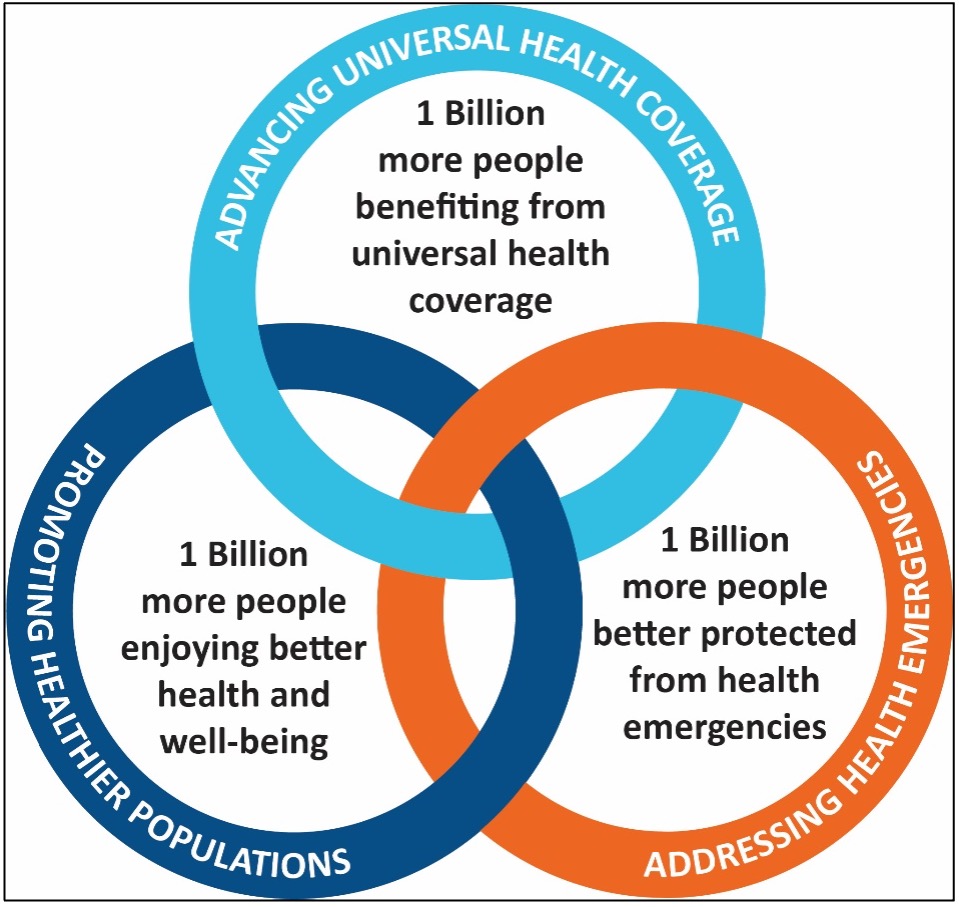
Fig. 12 (Adapted from WHO 2019d): The triple billion target of WHO’s GPW13.
Tobacco control also touches upon GPW13’s other two pillars: one billion more people with universal health coverage (UHC) and one billion more people better protected from health emergencies. This is because UHC can be financed through tobacco taxes, cessation services are an essential aspect of UHC, and a failure to address the tobacco epidemic decisively will lead to a crushing burden of NCDs that will undermine efforts to realise UHC, particularly in LMICs (WHO 2019a, d). As seen in the COVID-19 pandemic, tobacco control and NCD prevention and control agenda is also an important foundation to better protection from health emergencies (UN Interagency Taskforce 2020; WHO 2020; Kluge et al. 2020). People with underlying NCDs, such as tobacco-related diseases, will be much more vulnerable during communicable disease outbreaks (such as COVID-19) and they will also likely suffer from disruptions to public health programs and healthcare services that are needed for preventing and managing NCDs (Mehra et al. 2020; UN Interagency Taskforce 2020; Kluge et al. 2020).
Tobacco Control Implementation
Tobacco control’s prominence in the WHO Global Action Plan on NCDs (2013–2020), the UN NCD Agenda, the SDGs, and GPW13 is justified by both the success of the WHO FCTC’s 15 years of implementation and the formidable ongoing and emerging challenges it is still needed for. There are approximately 500 studies attesting to the efficacy of its measures when implemented (Zhou and Liberman 2018). Demand-reduction measures are the most widely and well implemented provisions of the WHO FCTC (Chung-Hall et al. 2018). Because of this, there is a substantial evidence base for their and the WHO FCTC’s efficacy with estimates of an average 1.57% decrease in smoking prevalence per demand reduction article implemented (Chung-Hall et al. 2018). As noted in section “Global Context of the Tobacco Epidemic”, there was a major expansion to supply-reduction side measures with the Illicit Trade Protocol, which came into force 13 years after the WHO FCTC, but at time of writing it has not had been in force for long enough to have had a measurable impact (NCI and WHO 2016; Chung-Hall et al. 2018). As noted in Box 6 above, combating illicit trade is an important component of global tobacco control because smuggled tobacco products undermine demand reduction measures and siphon off tobacco tax revenues (World Bank 1999). But, in general, supply side measures are not expected to result in a major impact on consumption because “if one supplier is shut down, an alternative supplier gains an incentive to enter the market” (World Bank 1999).
The MPOWER Package
MPOWER is an evidence-based technical package to help countries implement evidence-based demand reduction measures for tobacco control – in line with the WHO FCTC’s – developed by WHO and released in 2008 with Bloomberg Philanthropies’ support. The MPOWER technical package’s implementation is critical to recent and prospective success on tobacco control. There is a seamless relationship between the WHO FCTC and the MPOWER technical package: while the WHO FCTC is the definitive baseline for all tobacco control work, MPOWER provides the gold standard for achievement in implementing the WHO FCTC’s reduction measures. It calls for monitoring tobacco use (Article 20), protecting people from tobacco smoke (article 8), offering help to quit tobacco (Article 15), warning about the dangers of tobacco (Articles 11 and 12), enforcement of TAPS bans (Article 13), and raised tobacco taxes (Article 6). Implementation of these measures up to the best practice level is monitored by WHO and the effectiveness of Member State implementation is scored according to the level of achievement based on associated indicators (see Fig. 13, above, for details). Each indicator has a best-practice, highest level of achievement, target which all Member States are urged to work toward. Implementation of MPOWER is monitored for all WHO Member States, not just States Parties to the WHO FCTC. Global and country-specific progress on MPOWER is collated and published once every year two years in the biennial WHO Global Report on the Tobacco Epidemic. As seen in Fig. 14, in 2019, five billion people, 65% of the global population across 136 countries, were covered by at least one MPOWER measure at its highest level of achievement – when all the tracked indicators for an MPOWER measure fulfil certain best-practice conditions (WHO 2019a). This is a more than fourfold increase over 2007 when only one billion people were covered to this level (WHO 2019a). Of these five billion, 3.9 billion live in LMICs and a total of 61% of those living in LMICs are protected (WHO 2019a). These increases in MPOWER coverage and the consequent protection afforded people around the world is a demonstration of the WHO FCTC’s success. Figure 14 also breaks down MPOWER coverage in 2019 by measure. The only two countries to have adopted all MPOWER measures at a full level of achievement are Brazil and Turkey, middle-income countries – see Box 8, below (WHO 2019a).
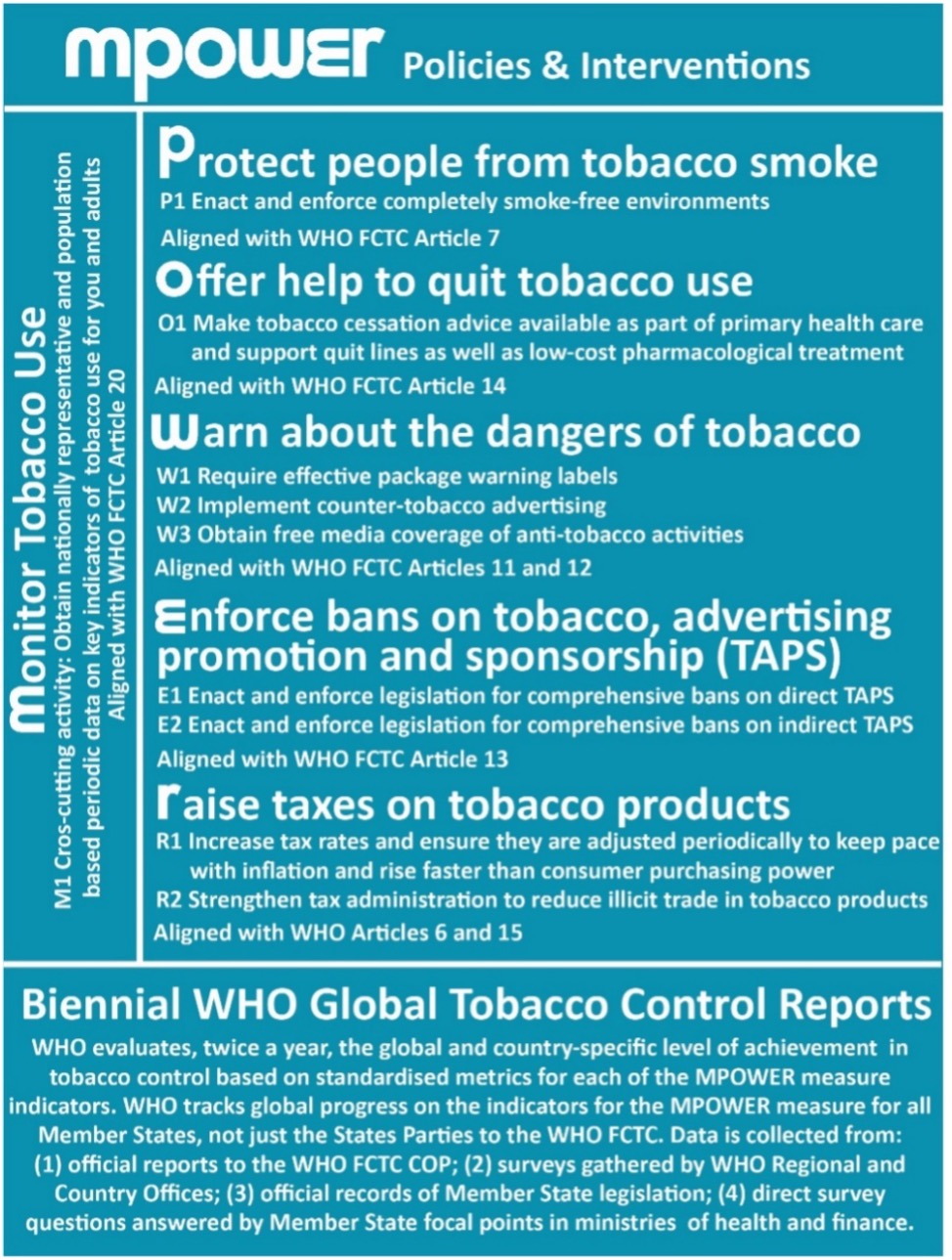
Fig. 13 (Adapted from WHO 2008): MPOWER measures, indicators, and tracking.
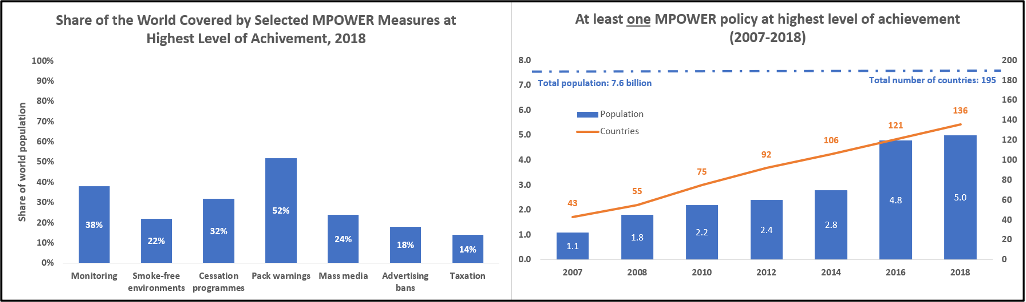
Fig. 14: MPOWER coverage. (WHO 2019a)
The policies included in the MPOWER package are highly cost-effective but still under-implemented (NCI and WHO 2016). There is a broad association between increased implementation of MPOWER measures and decreases in prevalence at the level of WHO Regions: those regions making the best progress on MPOWER policies are also seeing stronger declines in prevalence (WHO 2019b). For example, every country in the South-East Asia Region made progress on MPOWER measures between 2012 and 2018 and saw strong progress while the East Mediterranean region made the least prevalence reductions in a context of overall very slow progress on MPOWER policies (WHO 2019b). It is estimated that over 22 million premature deaths were averted between 2007 and 2014 by the implementation of the measures of the MPOWER technical package (Levy et al. 2018). The most cost-effective single measure is raising taxes and it is particularly effective with the more price-sensitive tobacco users of LMICs – a 10% price increase will reduce their consumption by at least 5% and up to 8% compared with about 4% in HICs – and price-sensitive youth whose entrance into potentially lifelong addiction is particularly important (WHO 2019a; Bettcher et al. 2015). It has been estimated that a $1 per pack (international dollars) excise increase in all countries would increase excise per pack by 80%, increase the mean retail price of cigarettes by 42%, decrease global cigarette consumption by 18%, and result in a relative prevalence decline of 9% (Goodchild et al. 2018). Despite this, it is also the measure least implemented at a high level of achievement (WHO 2019b). Even worse, cigarettes have become more affordable in many LMICs over the last three decades. Affordability is a product of the price of cigarettes, determined by, inter alia, inflation and tax rates, and growth or decline in incomes. Over the 1990s incomes rose in LMICs without proportionate rises in excise and, because of this, overall relative increases in affordability have been seen in LMICs and this continues to be the case for many countries (NCI and WHO 2016; WHO 2019a). By contrast, substantial tax rises outpaced inflation and income growth in HICs leading to decreases in cigarette affordability and overall higher levels of achievement in raising taxes than LMICs (NCI and WHO 2016; WHO 2019a). Because of this trend in affordability and the high cost-effectiveness of the measure, the World Bank has called for a tripling of excise taxes in most LMICs as a crucial measure for helping the world achieve the tobacco use prevalence reductions called for in the SDGs (Marquez and Moreno-Dodson 2017).
Box 8: MPOWER Best Practice in Turkey and Brazil
Turkey was, in 2013, the first country to achieve the highest level of achievement on every MPOWER measure and, in 2018, Brazil became the second (WHO 2019a). Both these middle-income countries evinced an early commitment to tobacco control and rapid uptake of the WHO FCTC, with both countries taking early action on ratification (WHO 2013, 2019a). Brazil, having been elected to chair the Intergovernmental Negotiating Body during the WHO FCTC’s negotiation, took the lead in rebutting claims that tobacco control was exclusively an HIC interest (WHO 2019a). Turkey, meanwhile, early after ratification distinguished itself with its monitoring programs being one of the first countries to complete the Global Adult Tobacco Survey (GATS) and was one of only two countries to repeat the survey soon after (WHO 2013). Another innovative policy was implementation of warning through mandates that broadcasters screen powerful programs in primetime television slots, and it also distinguished itself through thorough enforcement of its TAPS bans and other tobacco control policies (WHO 2013). Brazil’s rapid strides in ratifying and implementing the WHO FCTC are particularly noteworthy because it is one of the world’s leading tobacco leaf producers (WHO 2019a). Brazil led the world by becoming the first country with over 100 hundred million people to protect them by making all public and work places smoke free and the first large country to offer help to quit through including its national quit line number on all cigarette packs – provoking a major increase in calls that exceeded all other quit lines globally in that year (WHO 2019a).
These countries are exemplars of not only raising taxes and prices but doing so while decreasing consumption and increasing revenue – see Fig. 15, below. Of course, these decreases in consumption are also attributable to the other effective tobacco control measures implemented: measures of the MPOWER technical package, complemented by the rest of the WHO FCTC measures, are always more than the sum of their individual parts. That said, tax increases were an important part of the puzzle for both countries and have brought in revenue that will provide for public health financing and other important priorities. Because of this additional success, they are exemplars not only in the implementation of the comprehensive MPOWER package but also for its most effective single measure: raised taxes. Despite this success, these two countries still have some work to do in the enforcement of their bans on TAPS and smoking in public and indoor environments as well continuing to implement progressive excise increases to ensure, at a minimum, that tobacco does not become more affordable with income growth. On all the MPOWER measures, the highest level of achievement under the metrics does not constitute a ceiling for tobacco control and there is always room for improvement. Further, tobacco control is a marathon and not a sprint so countries need to enforce and update legislation and regulations if their efficacy is to be maintained.
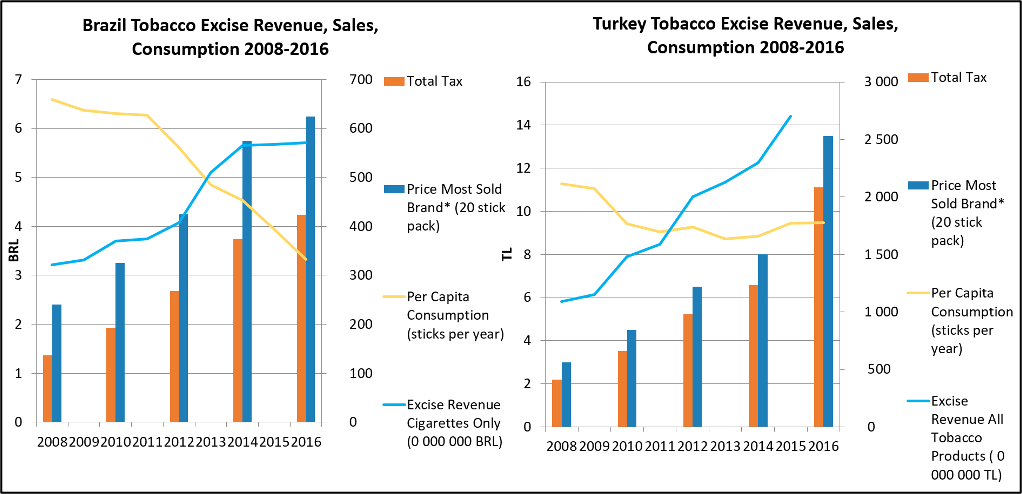
Fig. 15 (Adapted from WHO 2017)
As is seen in the case study of Brazil and Turkey – at Boxes 8 and 9 – tobacco taxes are not only effective demand reduction measures, but provide a substantial return at low cost, as little as US$0.05 per capita per year to administer in LMICs (WHO 2019a). As seen at Box 9, tobacco taxes raise revenue that can be invested into public health and other important priorities over the short-term because reductions in consumption are gradual and more than offset by the increased tax revenue (Marquez and Moreno-Dodson 2017; WHO 2019a). Over the medium- and long-term, revenues will likely decline as consumption causes the tax base of tobacco taxes to atrophy but revenue will, by then, be able to be drawn from the increased incomes and productivity that will result in an overall healthier population (Marquez and Moreno-Dodson 2017). In addition, reduced NCDs burden will mean public health expenditure that otherwise would be squandered treating tobacco-related disease can instead by diverted to prevention and treatment elsewhere in the public health system or to achieve other aspects of the SDGs (WHO 2018c).
Box 9: A Win-Win for Revenue and Health in Philippines
Philippines makes an interesting case study as a large grower of tobacco leaf and manufacturer of cigarettes that managed, in 2012, to enact and implement highly significant sustained tax rises and tax structure simplification that resulted in large revenue gains, consumption decreases, and increased spending on public health. In the face of industry opposition, the reform was achieved through a multisectoral whole-of-government and whole-of-society coalition. This included officials from the ministries of health and finance, key parliamentarians, civil society organisations, and medical professionals (WHO 2015). The tax’s revenue was devoted to funding a new universal health insurance plan for the most the vulnerable and with 15% dedicated to promoting alternative livelihoods for tobacco farmers and their communities – as per, Article 17 of the WHO FCTC (WHO 2015). Beyond being one of the largest increases in tobacco tax ever, its effect in reducing demand was ensured by its sustained nature with annual 4% increases established (WHO 2015). It was also paired with simplification of the tax structure that reduced opportunities for tax avoidance to increase effect on price as well as increase revenue (WHO 2015). The resultant increase to revenue exceeded expected gains by a factor of two within the first year after implementation and the revenue meant that, within three years, more than ten million poor people and their dependents had been brought into the health insurance system on subsidies, as referred to above (WHO 2015; Marquez and Moreno-Dodson 2017). The years since the tax rise have seen a sustained reduction in tobacco use prevalence associated with reduced demand (WHO 2017). Accordingly, the tax reform proves, as seen in Fig. 16, below, a win-win: a win for reducing tobacco demand and a win for public health’s financing (Marquez and Moreno-Dodson 2017; WHO 2015). It also provides a case study in how earmarking to a popular initiative can provide enduring support for even a very significant tobacco tax rise while also funding progress on the other SDGs, such as UHC (Marquez and Moreno-Dodson 2017). The Philippines has since enacted a further major tax reform, which was passed in 2019. This scheduled incremental increases in the rate between 2020 and 2023 that would result in a total 33% increase followed by annual increases of 5% from 2024.
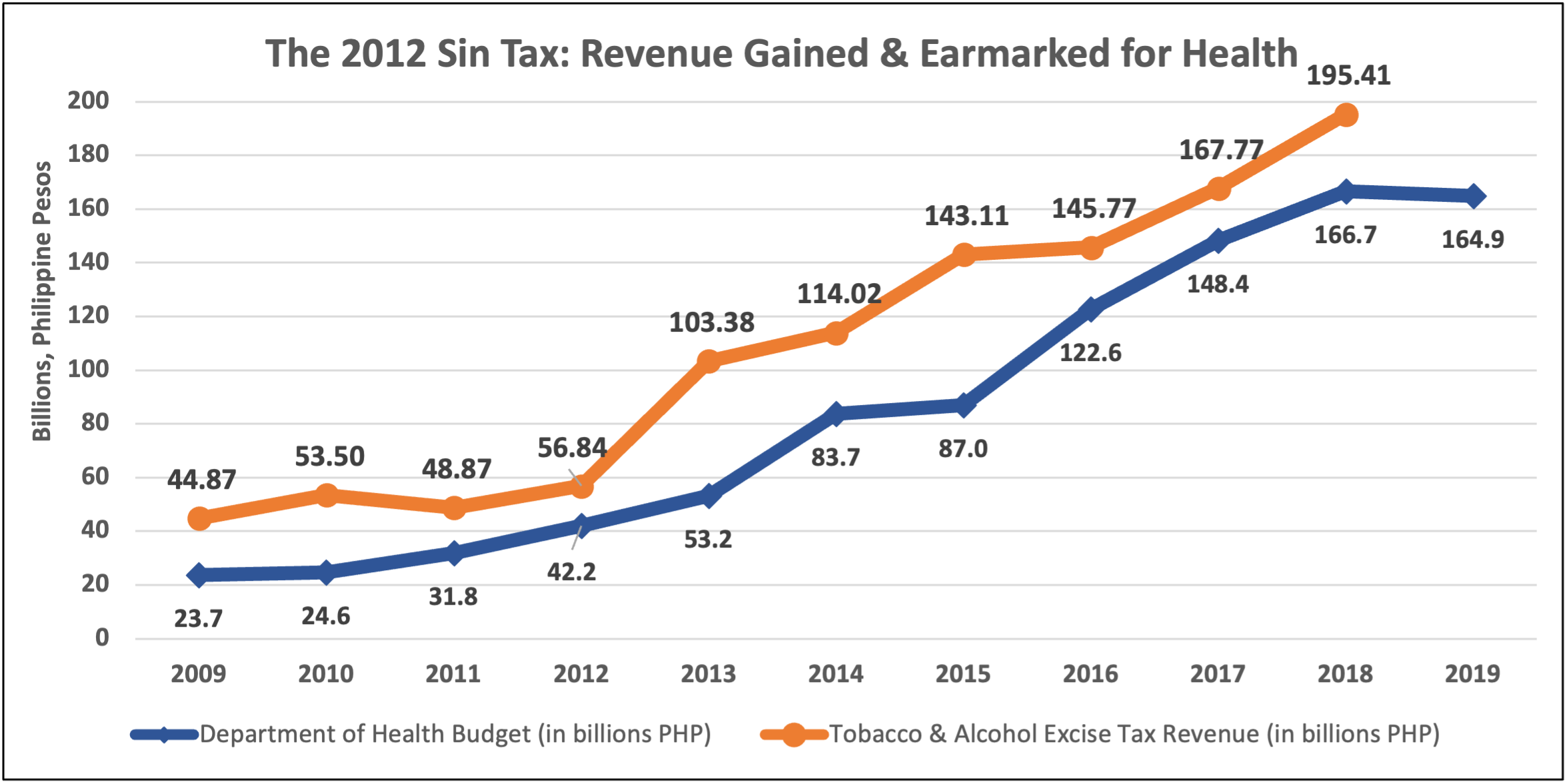
Fig. 16 (Data from Philippines Bureau of Internal Revenue): this data represents the revenue gained and earmarked from the entire Sin Tax which covered both tobacco and alcohol excise in the years depicted.
Implementing Article 5.3
One of the greatest barriers to tobacco control has been and remains industry interference (Minhas and Bettcher 2010). Combating industry interference through complete implementation of Article 5.3 has been a priority for WHO and the WHO FCTC Secretariat as well as both of their global partners. While the WHO FCTC COP has promulgated guidance on Article 5.3 and the Secretariat is tracking implementation, WHO has, in addition to monitoring patterns of industry interference, been providing technical assistance to Member States in their implementation of the Article and the COP Guidelines to it (Minhas and Bettcher 2010). Domestically, many countries have incorporated Article 5.3 directly into national legislation, such as Uganda, or in official guidelines for civil servants, such as the Philippines, but further implementation of Article 5.3 and its guidelines is still needed (Assunta 2018; Chung-Hall et al. 2018). In line with Article 5.3, industry has been entirely excluded from the UN system and its agencies have been urged to devise strategies to prevent industry interference (Bialous 2019). At the international level, proactive efforts have focused on monitoring and chronicling developments of industry tactics as well as exposing their proxies and surrogates (Minhas and Bettcher 2010). This ongoing work is needed to develop strategies to counteract industry interference but also operates to directly offset the millions spent by TTCs every year to rehabilitate their image by exposing their contrivances (Minhas and Bettcher 2010; Gilmore et al. 2015). Despite these efforts, industry interference by TTCs remains one of the greatest obstacles to WHO FCTC implementation as is discussed further in section “Partnerships for Action on Tobacco Control”, below (Bialous 2019).
Partnerships for Action on Tobacco Control
globalisation has introduced new actors onto the stage of global health diplomacy, including that of tobacco control (Bettcher et al. 2015). Consequently, the governance of global health is increasingly fragmented across overlapping regimes and actors unorganised in set hierarchies (Bettcher et al. 2015). There are new opportunities for negative actors, like the tobacco industry, to influence the global commercial determinants of health. But there are also opportunities for this influence to be counteracted by presently underutilised resources of newly visible positive actors, such as philanthropic groups, civil society organisations (CSOs), and the actors of subnational government (Bettcher et al. 2015). Because no single actor can succeed by itself in the contemporary landscape of global health governance, partnerships have been and will continue to be the foundation for success in tobacco control at all levels of implementation. Understanding how partnerships are formed through dynamic and dense webs of connections between disparate actors and coalitions is essential for understanding tobacco control and its future.
Partnerships Between Intergovernmental organisations
As a binding treaty for institutionalised tobacco control backed up by technical guidance from WHO, the WHO FCTC has been uniquely useful for facilitating coordination and cooperation between these actors. WHO and the WHO FCTC Secretariat are central nodes around which these emergent actors have formed networks for tobacco control in concert with conventional actors, such as states and other intergovernmental organisations. A bedrock for WHO FCTC implementation through these networks has been the relationship of mutual cooperation between the Convention Secretariat and WHO (Minhas and Bettcher 2010; McInerney 2019; Zhou and Liberman 2018).
Collaboration within the broader UN system on tobacco control has been a priority for WHO and the Convention Secretariat in their joint effort to promote the WHO FCTC and its implementation (McInerney 2019). The most notable success of this effort was the explicit incorporation of the WHO FCTC’s implementation into the SDGs as target 3.A as well as the preceding and subsequent elevation of tobacco control within the broader UN agenda at the three high-level meetings of NCDs at the General Assembly, which all called for the acceleration of WHO FCTC implementation (McInerney 2019). An immediate and significant outcome was the institutionalisation of cooperation on tobacco control and NCDs by the high-level meetings in the form of the UN Interagency Taskforce on NCDs. Comprising over forty intergovernmental organisations, including the Convention Secretariat, the taskforce is led by WHO and organised around implementation of the WHO Global Action Plan on NCDs (McInerney 2019). WHO and the Convention Secretariat have together ensured that the WHO FCTC and tobacco control receive particular attention in the Taskforce’s work (McInerney 2019). An important structural result of the Taskforce’s work was the creation of a draft policy on preventing tobacco industry interference across the UN system and its eventual adoption by the UN Economic and Social Council with the Taskforce positioned to monitor and encourage the policy’s full implementation (McInerney 2019; UN Interagency Force 2020). The Convention Secretariat chairs the Taskforce’s thematic group on tobacco control which has, since its establishment in 2017, been focused on promoting implementation of the WHO FCTC, the Illicit Trade Protocol, and the UN’s policy on tobacco industry interference as well as bringing its membership together in cooperation on promoting alternative and sustainable livelihoods for tobacco farmers – pursuant to WHO FCTC Article 17 (UN Interagency Taskforce 2020. One of the Taskforce’s most successful initiatives is “Be He@lthy Be Mobile,” as detailed in Box 10, below.
Box 10: Best Practice Collaboration: Be He@lthy Be Mobile
A joint-initiative of WHO and the International Telecommunication Union (ITU), as well as private sectors, governments, and academia, the “Be He@lthy, Be Mobile” consists of guidance and technical support for the implementation of national mobile health programs for preventing and controlling NCDs (UN Interagency Taskforce 2020). In the course of its six years, 16 programs in 12 countries have benefited from the initiative’s support in guidance, design, and implementation phases (UN Interagency Taskforce 2020). Successes include the mobile diabetes, mobile tobacco cessation, and mobile cervical cancer programs (UN Interagency Taskforce 2020). In India, the tobacco cessation program, “mCessation,” has reached over 2.1 million people and studies of its implementation provide early evidence of its efficacy in assisting people in quitting tobacco (WHO 2019a). The program has an average quit rate of 7% for both smokers and smokeless tobacco users within only six months of their enrolment (WHO 2019a). This is a particularly significant achievement because Article 14 of the WHO FCTC is one of the least implemented, and fewer countries have been offering tobacco users comprehensive help to quit (the O of MPOWER) than needed to reduce tobacco use prevalence significantly soon (WHO 2019a). The mCessation model has changed this by establishing a novel mechanism by which countries, in particular LMICs, can provide cessation support to a high level of achievement (WHO 2019a). Now its value has been proven in tobacco cessation – as well as diabetes management and cervical cancer prevention – there are ongoing efforts to scale up the initiative with the aim of reaching 100 million people with at least one of its programs (UN Interagency Taskforce 2020). There are also efforts toward providing more implementation handbooks and broader set of applications and data solutions to Member States (UN Interagency Taskforce 2020). To assist progress, this model partnership is exploring its extension with other UN agencies such as the UN Children’s Fund (UNICEF) (UN Interagency Taskforce 2020). The initiative provides a case study in how collaboration across the UN system can lead to gains needed for achieving the SDGs and progressing action on tobacco control.
Partnerships with and Between Non-state Actors
As noted in section “Global Context of the Tobacco Epidemic”, above, CSOs and academia played a crucial role in the WHO FCTC’s conception and negotiation. Implementation of the WHO FCTC has featured a similar need to rely on CSOs and academia. As set out at Article 4.7, “The participation of civil society is essential in achieving the objective of the Convention and its protocols.” organisations such as the Framework Convention Alliance (FCA), the NCD Alliance, the Campaign for Tobacco Free Kids (CTFK), the South-East Asian Tobacco Control Alliance (SEATCA), American Cancer Society (ACS), and the International Union Against Tuberculosis and Lung Disease (the Union) are crucial nodes in tobacco control networks for assisting implementation of demand reduction measures, facilitating tobacco product regulation, and monitoring tobacco industry tactics (WHO 2019a; Drope et al. 2018). Researchers and research institutes – see more in Box 11 below – are also key to tobacco control with, for example, notable contribution on tobacco industry tactics. More recently, Bloomberg Philanthropies (BP) founded STOP (Stopping Tobacco organisations and Products) in partnership with key CSOs and research institutes working on countering tobacco tactics: University of Bath’s Tobacco Control Research Group, SEATCA’s Global Centre for Good Governance in Tobacco Control, the Union, and Vital Strategies (WHO 2019a). STOP advances Article 5.3 by monitoring, chronicling, and exposing tobacco industry interference globally (WHO 2019a; Rojhani et al. 2019; Bialous 2019). The role of WHO and WHO FCTC Secretariat partnerships with academic and research institutes is analysed in Box 11, below.
Box 11: Partnerships Between Intergovernmental organisations and Research Institutes
WHO has entered into tobacco control partnerships with research institutes and universities since the late 1970s. This was achieved by formally designating 16 universities and research institutes, as WHO Tobacco Control Collaborating Centres (WHO TCCC), with now at least one being in each of the six WHO regions. While each WHO TCCC is focused on a specific overarching topic in tobacco control, they together cover nearly every aspect of the knowledge base needed for tobacco control. The partnership framework is particularly crucial in advancing WHO’s work in supporting its Member States to implement comprehensive measures for tobacco control and specifically in furthering the research and surveillance needed for tobacco product regulation and countering tobacco industry interference (WHO 2018a). Similarly, the Convention Secretariat has established Knowledge Hubs on various topics and tobacco industry monitoring centres – called “Observatories” – through partnership agreements with research institutes and universities across each of the six WHO regions (Zhou and Liberman 2018; Bialous 2019). With each focused on specific articles of the WHO FCTC, this partnership network helps inform the work of the Convention Secretariat and the guidance provided by the COP (Zhou and Liberman 2018). Together, WHO and the WHO Secretariat have established two globe-spanning networks that harness the potential of governmental and tobacco industry independent nongovernmental research institutes for tobacco control’s advancement – see Fig. 17, below.
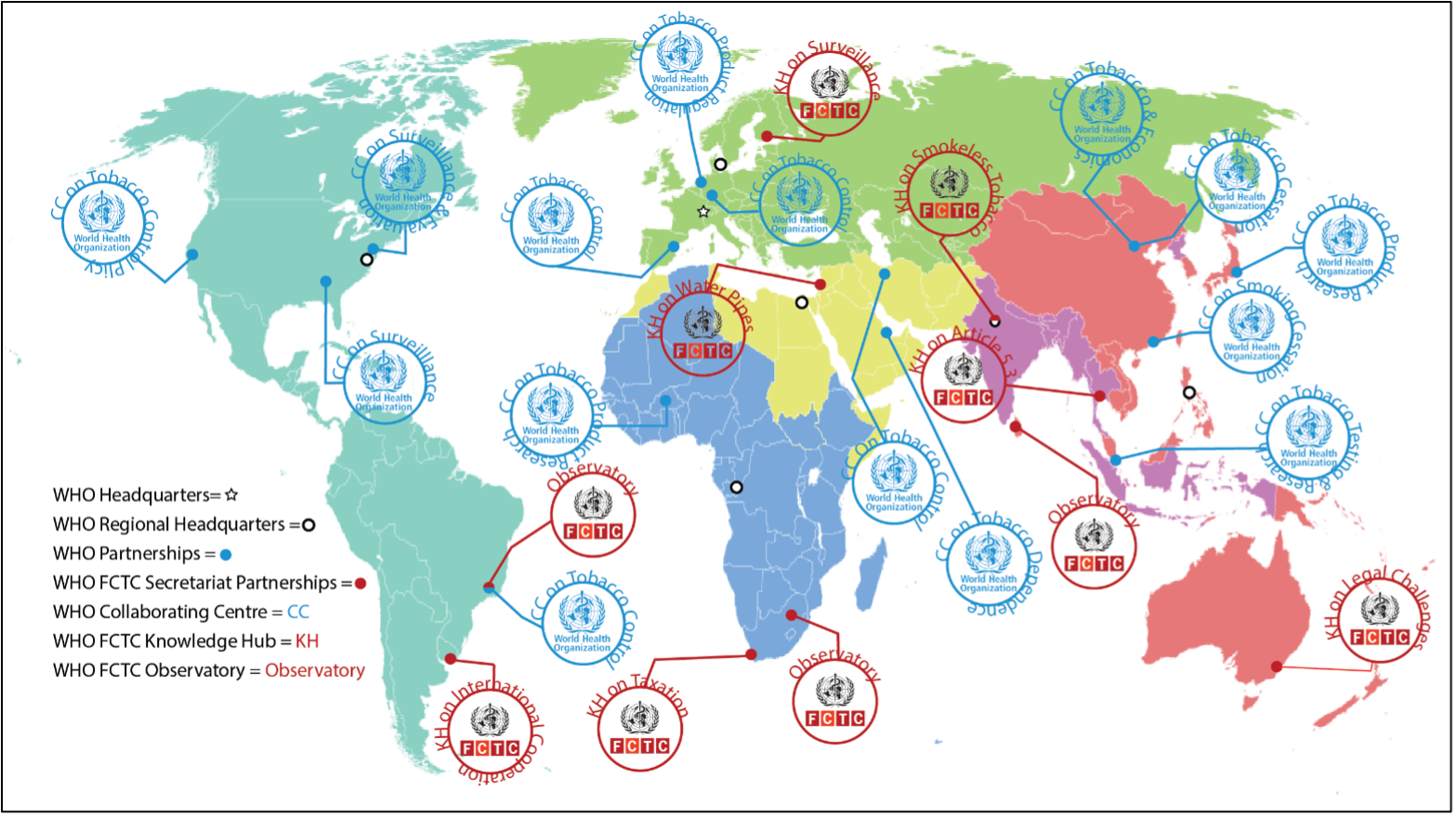
Fig. 17: WHO collaborating centres and WHO FCTC secretariat knowledge hubs and observatories
Philanthropies have more generally been crucial nodes in global and regional tobacco control networks, as well as interrelated networks for preventing and controlling NCDs. The partnership between Bloomberg Philanthropies and WHO has proven to be one of the most significant relationships in the WHO FCTC’s implementation and has committed funding of over US$1 billion for tobacco control (Rojhani et al. 2019; McInerney 2019). In 2006, Bloomberg Philanthropies founded the Bloomberg Initiative to Reduce Tobacco Use in partnership with WHO, CTFK, Vital Strategies, the John Hopkins Bloomberg School of Public Health, the Union, the University of Illinois’s tobacconomics program, and the CDC Foundation (Reubi 2016). The initiative has made numerous tobacco control grants with a focus on tobacco control in LMICs and, particularly, the ten large LMICs with greatest tobacco use prevalence (Reubi 2016; Mamudu et al. 2011). A key aspect of the partnership has been funding of the WHO’s MPOWER package for implementing the WHO FCTC’s key demand reduction measures (Gilmore et al. 2015; McInerney 2019). This has been underpinned by crucial support for the Global Adult Tobacco Survey (GATS) and Global Youth Tobacco Survey (GYTS) monitoring programs (Wipfli and Samet 2016; Reubi 2016). The evidence-based MPOWER package and the global monitoring programs have provided coherence to WHO’s technical assistance on WHO FCTC implementation and the Bloomberg Initiative’s overlapping tobacco control implementation networks.
The Gates Foundation have also collaborated with the WHO on tobacco control. They provided funding for tobacco control and in collaboration with WHO supported large-scale WHO FCTC implementation efforts to prevent the epidemic taking root in Africa as well as to combat it in Southeast Asia (Reubi 2016; Mamudu et al. 2011; US HHS 2014). This has included extensive funding to build up networks of support for civil society and researchers in these regions (Gilmore et al. 2015). One notable example from the first phase of the partnership is the establishment of the Centre for Tobacco Control in Africa by the WHO with support from the Gates Foundation (Centre for Tobacco Control in Africa 2020). The Centre advances the Gates Foundation priority of promoting health and sustainable development across the continent by providing WHO Member States technical support for tobacco control (Centre for Tobacco Control in Africa 2020).
Partnerships with and Between Municipal Governments
Another initiative of Bloomberg Philanthropies has been the establishment of the Partnership for Healthy Cities, in conjunction with Vital Strategies and WHO. Founded in 2017, the Partnership is a global network of 70 cities working on NCDs and injury prevention at the local level. It was formed against a backdrop of accelerating municipalisation of political action on health, and with many common risk factors linked to urbanisation, NCDs are a critical component of this work (see Box 12).
The Partnership draws upon WHO’s technical support packages, such as components of MPOWER, for high-impact and evidence-based measures in NCD and injury prevention (Krug et al. 2019). It does this while providing direct technical assistance for specific interventions and harnessing momentum through the sharing of guidance and good practices among municipal leaders within the network (Krug et al. 2019; Rojhani et al. 2019). Three of the 14 promoted interventions are tobacco control measures: raising taxes, enforcing TAPs bans, and protecting people with smoke-free law (Rojhani et al. 2019). Each mayor that joins the Partnership commits to work on a policy or program connected to one of its selected core NCD and injury prevention measures drawn from WHO’s technical packages, receiving technical assistance and a seed grant to support the work (Rojhani et al. 2019; Krug et al. 2019). Throughout the process cities share their experiences with peers and experts, thereby contributing to global understanding of the efficacy of local action on NCD and injury prevention, while also inspiring other municipal leaders to follow their example and protect public health (Rojhani et al. 2019).
Box 12: The Municipalisation of Tobacco Control and Action on NCDs
Over half of the global population now lives in a city and virtually all countries are becoming increasingly urbanised (Krug et al. 2019). As a result, cities are increasingly seen as a primary implementation site for policies to advance progress in achieving the SDGs, including action on NCDs and tobacco control (Krug et al. 2019). The importance of urban health is specifically recognised in goal 11 of the SDG’s call for cities to be made inclusive, safe, resilient, and sustainable (Krug et al. 2019). This is complemented by the call, under WHO’s Thirteenth Global Programme of Work, to promote health in all settings and support health diplomacy with municipal bodies (WHO 2019d).
The first WHO Healthy Cities network was established in 1988, and since then each regional office has developed its own branch of the initiative (WHO 2019d). There is consequently a legacy of experience with city health diplomacy and the cross-pollination of best practice (WHO 2019d). Developing similar transnational networks for cooperation between municipalities will be crucial to strengthening tobacco control. As the epidemic migrates to LMICs, cities in these countries are also appearing at the frontline of global tobacco control, especially around efforts to combat industry influence and other commercial determinants of health.
Negative commercial determinants of health are easily fostered within cities, due to higher incomes and greater consumer accessibility for the products and marketing tactics of multinationals when compared with rural areas (Rojhani et al. 2019). Rapidly growing cities in LMICs are particularly vulnerable because their more fragile social safety nets and public health systems may be less able to manage the burden of increasing mortality and morbidity from NCDs (Rojhani et al. 2019). Moreover, many LMICs lack the legal, social, and physical infrastructure needed to counteract and offset commercial influence (Rojhani et al. 2019). But as well as creating challenges for health, urbanisation also offers opportunities (Krug et al. 2019). By placing major public health issues directly under the supervision of leaders well-positioned to act on them, urbanisation has the potential to engender higher-impact public health interventions (WHO 2019e; Krug et al. 2019). In certain respects, municipal leaders are in a particularly strong position for implementing policies to prevent and control NCDs. Examples can include cross-cutting mandates between health and non-health issues (such as public transport or urban planning); the ability to act rapidly; ownership of relevant infrastructure; proximity to local communities; working relationships with key civil society and community volunteer organisations; and the ability to pilot schemes to establish a blueprint for national implementation (WHO 2019e).
The power of cities was recognised in a landmark of city health diplomacy: the 2016 Shanghai Declaration, which adopted by over one hundred mayors from around the world at the Ninth Global Conference on Health Promotion (Krug et al. 2019). The declaration recognised: (1) that good governance and whole-of-government approaches are crucial for health and a particular concern in improving the commercial determinants of health to combat NCDs – needed if fiscal policies and regulation are to be enacted; (2) encouraging health literacy, as seen in WHO FCTC article 12, is an important determinant of health; (3) community mobilisation is a necessary ingredient for successful action; and (4) city policymaking and city health diplomacy can promote health by fostering action for multiple SDGs (Shanghai Declaration 2017; WHO 2019a; Krug et al. 2019). The accompanying Shanghai Consensus went further to recognise ten priority areas for city health action including, alongside action on other NCD risk factors, the need to make cities smoke-free and also implement comprehensive bans on tobacco advertising, promotions, and sponsorship (International Mayors Forum 2016).
The Road Ahead: Current and Future Challenge
Challenge One: Tobacco Industry Litigation Under International Obligations
The defeat of three major international legal challenges to tobacco packaging regulations in the 2010s – see Boxes 13 and 14, below – marked an important shift in the stature of public health vis-à-vis international economic law that is largely, although not wholly, attributable to the WHO FCTC and its implementation (Bettcher et al. 2015; Nikogosian and Kickbusch 2018). In the 1980s through 1990s, the new economic order in international trade, investment, and intellectual property law was a tool the tobacco industry could manipulate (Bettcher et al. 2000; Minhas and Bettcher 2010). During this period the United States, where the industrial sector, including the tobacco industry, pressured many countries to open their markets to trade – in particular through using the 1974 US Trade Act’s Section 301 powers. The United States launched a trade law challenge against Thailand in Thailand – Restrictions on the Importation of and Internal Taxes on Cigarettes (1990) challenging Thailand’s import restrictions on cigarettes and other tobacco products, while allowing domestic production, under the 1947 General Agreement on Tariffs and Trade (GATT) as a discriminatory barrier to trade (GATT Panel 1990). Thailand argued that this measure was necessary to protect human health but the GATT Panel found that the import restrictions were not necessary and that other less trade restrictive alternatives, such as nondiscriminatory excise taxes and advertising restrictions, would be effective for that purpose (GATT Panel 1990; Bettcher et al. 2000). As a result, Thailand was able to move forward to implement these effective nondiscriminatory demand reduction measures, thus becoming a global tobacco control leader.
But legal threats by industry could also suffice to exert regulatory chill – see Boxes 13 and 14 for case studies. Major transnational tobacco companies collaborated to disseminate consistent legal arguments against tobacco plain packaging (TPP) and large graphic health warnings and threaten to bring proceedings that, if successful, could make governments liable for huge damages and costs. BAT, Rothmans, PMI, Reynolds Imperial Tobacco, and other major actors formed a working group, the “Plain Pack Group,” in 1993 to collaborate on legal strategies based around protections international economic law might arguably offer their intellectual property, investments, and rights under multilateral trade agreements – relying on the newly established 1994 GATT and 1995 TRIPS regimes (Crosbie and Glantz 2014). These legal arguments were repeatedly dismissed as weak in confidential advice from counsel, consultants, intergovernmental organisations, and government agencies the tobacco industry sought support from (Crosbie and Glantz 2014). Despite this, in the 1990s, industry deployed these weak legal arguments to convince Canada’s government and parliament to drop, for a time, TPP proposals they had been led to believe by the industry would expose them to massive legal liability (Crosbie and Glantz 2014). This is despite repeated advice given to the industry that these arguments were unlikely to succeed so governments were unlikely to incur liability (Crosbie and Glantz 2014). These episodes throw into relief how the crystallization of international economic law (in the fields of international intellectual property, trade, and investment law) in the WTO dispute settlement system and investor-state dispute arbitration systems was not accompanied with sufficiently clear protections for public health measures. Provisions in each system expressly provided for exceptions from general rules for legitimate public health measures but, particularly, in the 1990s and early 2000s, there was concern for how the protections would be interpreted and applied when relied on in a defence of an innovative tobacco control measure (Crosbie and Glantz 2014; Bettcher et al. 2000).
The WHO FCTC disrupted international economic law’s hegemony through its establishment of a competing set of legal norms protective of tobacco control measures from a public health perspective (Nikogosian and Kickbusch 2018). It marked, alongside the Doha Declaration and eventually the SDGs and Illicit Trade Protocol as well, a counter-reaction to a globalisation that failed to fully incorporate the intrinsic and instrumental value of human health (Bettcher et al. 2000, 2015; Nikogosian and Kickbusch 2018). Although the machinery of international economic law remained susceptible to industry manipulation, levers for resisting these forms of exploitation were now available to tobacco control proponents (Minhas and Bettcher 2010; Zhou and Liberman 2018). While not explicitly included in the WHO FCTC, such measures are implicit in its text (Zhou and Liberman 2018).
Box 13: Philip Morris v Uruguay (2016)
In 2009 Uruguay sought to strengthen its tobacco control laws and implement Articles 11 and 13 of the WHO FCTC through a decree including the following measures (1) increasing the size of graphic health warnings to cover 80% of cigarette packages; and (2) a single presentation requirement precluding tobacco manufacturers from marketing more than one variant of cigarette per brand family (Philip Morris v Uruguay 2016). In response, three Philip Morris companies challenged the above measures under a bilateral investment treaty between Switzerland and Uruguay (BIT), claiming that Uruguay had breached the terms of the BIT, including by: expropriating the claimants’ investment in the country (i.e., deprived the claimants’ business in the country of significant value); denial of fair and equitable treatment; impairment of the use and enjoyment of the claimants’ investments; and failure to observe commitments as to the use of trademarks, claiming damages of USD22.3 M. Uruguay responded that the Challenged Measures were adopted in compliance with Uruguay’s international obligations, including the BIT, for the single purpose of protecting public health. (Philip Morris v Uruguay 2016). In July 2016 – after five years of extensive argument and submission of evidence and tens of millions of USD in expenses incurred by Uruguay and supported by Bloomberg Philanthropies – all of the challenges were dismissed and the claimants ordered to pay USD7M toward Uruguay’s costs (Phillip Morris v Uruguay 2016). In finding that there had been no breach of the standard for fair and equitable treatment, the arbitral tribunal relied heavily on 2 amicus curiae submissions, one by the WHO and WHO FCTC Secretariat, and another by the Pan-American Health Organization, based on the WHO FCTC and COP guidelines, which provided evidence that the measures were reasonable, evidence-based, effective and implemented as part of a duty to protect public health (Phillip Morris v Uruguay 2016). The award underscored the importance of the WHO FCTC in setting tobacco control objectives and establishing the evidence base for measures.
The emergence of the WHO FCTC was not, however, a matter of conflict between norms of public health and the norms of international economic law (Kicksbuch et al. 2018). States retain their sovereign and police powers to regulate to protect public health and the WTO trade agreements, treaties on intellectual property rights and (to varying extents) international investment agreements, contain exceptions, flexibilities, and carve outs – this can cause other obligations to yield to the priority for public health retained through these exceptions and flexibilities, which is advanced by the WHO FCTC (Nikogosian and Kickbusch 2018; Zhou and Liberman 2018). But this dynamic compatibility only applies when the other strictures of these international economic law instruments are met (Kicksbuch et al. 2018). Governments can strengthen their legal position against challenges by implementing measures that are aligned with the obligations, purposes, and evidentiary basis of the WHO FCTC or the COP’s guidance on the implementation of its articles and are drafted to meet the conditions of any exemptions and flexibilities available under applicable trade and investments agreements to which the government is party. This is all much easier said than done: even with the WHO FCTC as a counterbalance, international economic law still imposes a formidable burden on countries with limited specialist legal capacity and resources (McGrady 2018).
Box 14: Australia – Tobacco Plain Packaging at the WTO
The WHO FCTC does not specifically oblige States Parties to implement tobacco plain-packaging (TPP). However, TPP is recommended in both the WHO FCTC COP’s 2008 Guidelines for the Implementation of Articles 11 and 13 as a means of giving effect to Parties’ obligations under those Articles (WHO FCTC COP 2008a, b). The Article 11 Guidelines recommend adopting measures to restrict or prohibit the use of logos, colours, brand images, or promotional information on packaging other than brand names and product names displayed in a standard colour and font style (plain packaging), to increase noticeability and effectiveness of health warnings and messages and address misleading industry package design techniques suggesting that some products are less harmful than others (WHO FCTC COP 2008a). The Article 13 Guidelines elaborate on the meaning of a “comprehensive” TAPS ban and how Parties may fulfil their obligation under Article 13 to implement such a ban (WHO FCTC COP 2008a). The Guidelines recommend as follows: “Packaging and product design are important elements of advertising and promotion. Parties should consider adopting plain packaging requirements to eliminate the effects of advertising or promotion on packaging. Packaging, individual cigarettes or other tobacco products should carry no advertising or promotion, including design features that make products attractive” (WHO FCTC COP 2008b).
This idea preceded the WHO FCTC with, as noted above, Canada and others having investigated its implementation in the 1990s before being dissuaded by spurious legal threats disseminated by the tobacco industry (Crosbie and Glantz 2014). When a TTP measure was eventually passed into law by Australia, the first in the world, coming into force in 2012, the tobacco industry and its surrogates brought proceedings in three different forums alleging that the measure breached international obligations under trade and investment agreements and domestic constitutional requirements (Zhou and Liberman 2018). Philip Morris Asia’s challenge under the investment agreement was dismissed by an arbitral tribunal on jurisdictional grounds and the Australian High Court also dismissed Japan Tobacco International’s constitutional challenge (Zhou and Liberman 2018).
The third legal challenge to Australia’s TPP law was brought in the WTO. With tobacco industry financing and assistance for all but one, four WTO members – all tobacco growing or producing countries but without major exposure to the Australian market – launched WTO dispute settlement proceedings (Gilmore et al. 2015; Vital Strategies 2019; Zhou and Liberman 2018). The core claims were that the Australian TPP measures: (1) were inconsistent with Article 2.2 of the Agreement on Technical Barriers to Trade (TBT Agreement) on the basis that they were more trade-restrictive than necessary to achieve a legitimate objective; and (2) were inconsistent with intellectual property protections under Articles 15.4, 16.1, 16.3, and 20 of the Agreement on the Trade Related Aspects of Intellectual Property Rights (TRIPS Agreement) (WTO Panel 2018). In its decision published on 28 June 2018, the WTO Panel found that the complainants had not demonstrated that the TPP measures are inconsistent with the TBT Agreement, TRIPS Agreements (or other treaties claimed).
The WHO FCTC and the COP’s guidelines on Articles 11 and 13 were accorded substantial weight by the Panel even though only one of the four complainants were party to the WHO FCTC (WTO Panel 2018). An Amicus curiae brief submitted by the WHO and WHO FCTC Secretariat was also influential in the Panel’s decision (WTO Panel 2018). The Panel cited the WHO FCTC and/or its Guidelines on the implementation of Articles 11 and 13 including: (1) in confirming the legitimacy of the objective being pursued by Australia of improving public health by reducing use of and exposure to tobacco products; (2) to support its characterisation of tobacco plain packaging as part of a comprehensive and multifaceted approach to tobacco control; (3) provided evidence on the nature of TPP measures and how, as they were to be implemented as part of a comprehensive package, the measures proposed by the complainants to serve as less trade restrictive alternative measures – such as an increase in the purchasing age to 21, education campaigns tobacco taxes or pre-approval for packaging and branding – were complements rather than alternatives; (4) noting that Australia had followed the recommendations in the WHO FCTC guidelines to confirm its finding that plain packaging was not an “unjustifiable encumbrance” on the use of trademarks in the course of trade (WTO Panel 2018). The legal validity of the Panel’s conclusions was confirmed by the WTO’s Appellate Body in June 2020 (WTO Appellate Body 2020).
Even before this, however, Australia’s success at the Panel stage had emboldened other countries to act: between Australia’s introduction of TPP and the Appellate Body’s ruling, similar measures have been legislated for in France, the United Kingdom, New Zealand, Norway, Ireland, Thailand, Uruguay, Saudi Arabia, Slovenia, Turkey, Israel, Canada, Singapore, Belgium, and Hungary with even more projected to join this list in the coming years (CTFK 2020; WHO 2019a). The conclusion of this legal saga marks a major victory for tobacco control efforts globally and a vindication for the impact of the WHO FCTC.
Even though these challenges were unsuccessful, and many countries have since passed TPP legislation without suffering any legal challenges, the industry arguably gained a partial victory by simply delaying action and opening up a new avenue for industry interference. Where before challenges based on international obligations had only been threatened, now these threats had been acted upon. The mere initiation of these legal challenges is known to have caused short-term delay to regulations in some countries and may have instilled a long-lasting regulatory chill by shifting the political economy of tobacco control regulation toward more conservative postures (Crosbie and Glantz 2014; Vital Strategies 2019; Bialous 2019). This is because the financial resources and political capacity needed to defend challenges under international obligations are formidable (McGrady 2018). Victory comes at a cost and is not guaranteed, while the costs in defeat, like compensatory relief, are even greater yet (McGrady 2018). The shell-game tactics of industry sometimes means that their failure comes with a contingent consolation prize. This same pattern is present in tobacco product regulation’s ongoing challenges and the tobacco industry’s resuscitation of the “harm reduction” paradigm for novel nicotine and tobacco products.
Challenge Two: Tobacco Product Regulation
Tobacco products are, still, exceedingly under-regulated compared with similarly hazardous consumables that are subject to regular and strict regulatory requirements by authorised agencies (WHO 2018a). This is despite Articles 9 and 10 obligations under the WHO FCTC for regulation of the contents and emissions of tobacco products and their disclosures, as well as the COP’s partial guidelines on these two Articles (WHO 2018a). A recent assessment concluded that these two Articles have seen some of the least progress in implementation out of any of the WHO FCTC’s measures (Chung-Hall et al. 2018). They have not, as originally envisaged, yet led to the erection of an international regulatory framework capable of piercing the insulated silos of tobacco product design guarded by tobacco industry (Minhas and Bettcher 2010; WHO 2018a). Without full implementation of Article 9 and 10 of the WHO FCTC, there would be vulnerability to industry interference in tobacco control contrary to Article 5.3 (WHO 2018a).
This is not for lack of effort on the part of WHO and the WHO FCTC Secretariat, as regulatory freedom is jealously guarded by industry to ensure it can keep its products on the market by all means and exploit product characteristics to make them more appealing to younger generations (WHO 2018a). WHO has been a big player in tobacco product regulation even prior to the entry into force of the WHO FCTC, with its establishment of the ad hoc Scientific Advisory Committee on Tobacco Product Regulation (SACTob) in 2000 to help facilitate tobacco product regulation and inform negotiations on the WHO FCTC (Minhas and Bettcher 2010). SACTob evolved into the WHO Study Group on Tobacco Product Regulation (WHO TobReg), in late-2003, with the WHO FCTC’s conclusion (Minhas and Bettcher 2010) and its work was later complemented by the WHO Tobacco Laboratory Network (WHO TobLabNet). WHO TobReg provides recommendations on evidence-based methods to the WHO Director-General for filling regulatory gaps in tobacco product regulation while WHO TobLabNet aims to strengthen global capacity in tobacco product testing and research (Minhas and Bettcher 2010). In 2006, following its establishment, the Convention Secretariat was directed by the COP to cooperate with WHO on product regulation and the latter was encouraged to continue its work on tobacco product regulation (Minhas and Bettcher 2010; WHO 2018a).
Some of the barriers to full implementation of Articles 9 and 10 of the WHO FCTC in line with the COP’s partial guidelines on Articles 9 and 10 and the WHO’s recommendations include: (1) limited understanding of best practices; (2) lack of adequate resources; (3) insufficient technical capacity; (4) lack of full appreciation of the value of tobacco product regulation (WHO 2018a). The Partial Guidelines have elaborated the regulatory provisions for attractiveness, which is one of the drivers for motivation to use tobacco products but have yet to elaborate the provisions relating to the toxicity and addictiveness of tobacco product (WHO 2018a). But Parties are at liberty to go beyond the measures elaborated in the Partial Guidelines or the Articles, as stated in Article 2 of the WHO FCTC, by adopting additional and stronger measures and some countries have exercised this right (WHO 2018a). Stepped up implementation of these Articles is urgently needed, not only to address toxicity and addictiveness of tobacco products but to also support full and comprehensive implementation of the WHO FCTC’s other articles. It would also act as a counter-weight to tobacco industry innovation of these products (WHO 2018a). In addition to assistance through the WHO coordinated TobLabNet and TobReg, the more recently established Global Tobacco Regulators Forum (GTRF) means there is now a network for cooperation and exchange of best practice among regulators and across countries (WHO 2018a).
Challenge Three: Novel and Emerging Nicotine and Tobacco Products
Ever since policymakers and the public began to grasp the fact that tobacco is inimical to human health and well-being, the tobacco industry has innovated “solutions.” This has seen the evolution of filter tip cigarettes – “the doctor’s choice” – into ventilated filter “light” cigarettes and, in the 1990s, smokeless tobacco (Bialous and Glantz 2018; Evan-Reeves et al. 2020). Secret documents show that tobacco industry interest in such products has, as might be expected, centred more on the potential for their innovations to increase profits, draw more people into the nicotine market, and stop current consumers from leaving (Evan-Reeves et al. 2020). The actual extent of “harm reduction” is unimportant to the industry when it can market its products as “less harmful” on the back of whatever science can be fabricated (Evan-Reeves et al. 2020; Bialous and Glantz 2018). Against a backdrop of tightening tobacco control regulations and declining cigarette sales in the industry’s key high-income and upper-middle-income markets, this playbook of innovating for “harm reduction” has been dusted off and is being recycled with the industry’s introduction and acquisition of novel and emerging nicotine and tobacco products – see Box 15, below (Evan-Reeves et al. 2020).
These products fit broadly into three categories: (1) electronic nicotine delivery systems (ENDS); (2) electronic non nicotine delivery systems (ENNDS); and (3) heated tobacco products (HTPs). Whereas HTPs are merely tobacco products with a new delivery system, ENDS and ENNDS (also known as e-cigarettes or vapes) contain no tobacco and instead aerosolize a liquid which may contain nicotine in the case of ENDS and not contain nicotine, in the case of ENNDS and other compounds (WHO 2019a).
HTPs have existed since the 1980s but only became popular in 2015 with the introduction of new generation products (WHO 2019a). They are the creation of the tobacco industry and three of the four major transnational tobacco companies (TTCs) have their own HTP brands (Evan-Reeves et al. 2020). Evidence on the impact of this newest generation of HTPs may have on health is sparse with much of what is being produced by industry to support their “harm reduction narrative” (see Box 15, below), and accordingly tainted by conflict of interest (WHO 2019a; Bialous and Glantz 2018). On the whole, available evidence suggests they are no less harmful than cigarettes and may be more harmful at a population level if they attract those who would not have used tobacco had they not been on the market or would have quit tobacco use in their absence (WHO 2019a). Because they are tobacco products, it is impossible to quit tobacco use by swapping from other tobacco products to HTPs (WHO 2019a; Ghebreyesus 2019). There is evidence that HTPs are heavily marketed to youth and much of the growth in their use has been driven by never-users rather than smokers swapping over from cigarettes in some jurisdictions (Evan-Reeves et al. 2020). There is also evidence to suggest that many users of HTPs also use them alongside other tobacco products, making them complementary products, with users being prone to exposure to the emissions of two or more products (Evan-Reeves et al. 2020; WHO 2019a).
The evidence on ENDS, which have been marketed since 2005 in some countries but only gained popularity in the last decade, is inconclusive and longitudinal studies are required (WHO 2019a). As ENDS began to prove highly popular, the tobacco industry moved in and began acquiring successful independent brands and introducing their own versions of the products (WHO 2019a; Evan-Reeves et al. 2020). At this time, the tobacco industry began to propagate the “harm reduction” narrative and framing of these devices (see Box 15, below). They are not, however, only marketed as less harmful but also sold to the public with the claim that they can assist with cessation in a way similar or even superior to evidence-based nicotine replacement therapy, such as nicotine patches (WHO 2019a). There is, however, insufficient evidence to support the claim that ENDS can assist tobacco users in quitting and, in the absence of this evidence, the promotion of these products as cessation aids could cause harm if it diverts those seeking to quit tobacco away from proven cessation aids and techniques (WHO 2019a). Attempts to study their effects on health are made more difficult by the variety of different ENDS and ENNDS and their variety of designs, some of which are prone to manipulation, as well as customisable and compositions of aerosolised liquids (WHO 2019a). It is, however, clear that ENDS are addictive and harmful to human health, contain a number of toxic compounds and are associated with an increased risk of cardiovascular diseases and lung disorders (Ghebreyesus 2019). Another issue, for both their effects on health and potential as cessation devices, is dual and poly-use, which is when these products are used with one or more tobacco products, a behaviour which happens to be the most prevalent form of the use of ENDS (Ghebreyesus 2019; WHO 2019a). There is also concern that these products may have a gateway effect: initiating never-smokers and youth into nicotine and then drawing them into use of tobacco products (WHO 2019a). This concern is further exacerbated by the extensive evidence of attempts to attract youth to these products with fun, colourful adverts featuring young people, sleek discreet designs and a variety of fruity and sweet flavours (WHO 2019a). There is some evidence to suggest these strategies have been successful with high youth uptake and a gateway effect among youth users (Evan-Reeves et al. 2020). Overall, there is particular concern for their population effects, but this may vary by regulatory context (Evan-Reeves et al. 2020).
Box 15: “Harm Reduction”
As a tobacco industry fabrication, “harm reduction” helps to sustain the conflation of ENDS and ENNDS and HTPs. By treating both products as similar “reduced-risk” or “harm-reduction” products in press releases, marketing and lobbying to policymakers, the tobacco industry argue for more favourable regulatory treatment for HTPs by presenting them as non-tobacco products and, in doing so, subvert the WHO FCTC. The harm-reduction frame is an effective way of misleadingly marketing HTPs to consumers as “safe” or, at least, “safer” and capturing and profiting off consumers, in particular youth, who would otherwise have never joined the nicotine market, as well as retain those who might have quit. It is also an effective way of blinding policymakers to the potential population level effects of ENDS and ENNDS by encouraging them to instead focus on the harm caused by the product on the individual.
This is a misapplication of the basic sense of “harm reduction” taking a public health approach – as seen in its use in relation drug dependence and its nexus with communicable disease – to only focus on harm to the individual to the neglect of harm to others and broader population-level effects. In real harm reduction policies, there is an attempt to deglamourise the product and restrict its uses to the necessary. This can be seen in safe injection sites, needle exchanges, and methadone programs. In each, there is care taken to target current users, whilst minimising or restricting access to others, and the services are packaged in a straightforward and accessible but essentially medical fashion. The programs are not promoted to the general public or packaged in a manner that could make them appear to be attractive to nonusers. Nor are the programs put in the hands of the principal vector for drug use, suppliers, in this case the tobacco industry but rather handled by government providers or licensed NGOs. The advocates of harm-reduction through ENDS, ENNDS, and HTPs, by contrast are, in general, happy with the tobacco industry handling this “harm reduction service.” These supporters of harm reduction also do not object to the products being promoted using fashionable, colourful, and widely advertised products that target young people who may or may not be current tobacco users (Lancet 2019). The reason why there is no objection is because the industry and its front-groups only want the façade of harm reduction: they want a chaotic form of harm reduction which serves their profit-making interests. What is needed instead is a public health approach to ENDS and ENNDS that aligns its treatment with that of cigarettes (Lancet 2019).
Tobacco harm reduction, under the guise of supporting public health, serves a perhaps more important end than the actual sale of these novel and emerging nicotine and tobacco products. Important as they are as a source of high-margin profit in otherwise declining markets, ENDS, ENNDS, and HTPs represent an exceedingly small share of revenue, around 3% of the total, when compared with cigarettes which make up most of the other 97% (Evan-Reeves et al. 2020). What matters more for industry is to be able to promise a future in which its products are not causing the deaths of hundreds-of-millions of people so that they may rehabilitate their image – seeming to be part of the solution rather than the core of the problem (Gilmore et al. 2015; Bialous and Glantz 2018; Evan-Reeves et al. 2020). PMI has been particularly eager to reap harm-reduction’s dividends through unbelievable attempts to claim it wants to “quit smoking too” while selling hundreds-of-millions of cigarettes a year and seeking to subvert tobacco control through aggressive litigation, marketing to youth and attempts to expand its market share (Evan-Reeves et al. 2020).
It has also committed to spending one billion USD over 12 years funding a new captive organisation, the Foundation for a Smoke Free World (FSFW) – PMI is its sole funder – to reproduce and launder its harm-reduction message. By using PMI’s money to fund “science” and “tobacco control researchers” around the world, the FSFW has been effective in capturing a large enough share of the tobacco control community that it can appear as though it is suffering from a “split” and that science and evidence on policy is unsettled (Evan-Reeves et al. 2020; Bialous and Glantz 2018). This undermines tobacco control on issues beyond these novel products with many of these researchers recycling industry talking points to castigate tobacco taxes as ineffective and criticise other proven effective tobacco control (Evan-Reeves et al. 2020).
Conclusions
Whenever the tobacco industry locks someone into long-term addiction, that person will lose, on average, a decade of life and the industry will gain, on average, US$10,000 in profit over that person’s abbreviated lifespan (Marquez and Moreno-Dodson 2017). This is their business model: they extract incredible profits by globalising commercial determinants of health devastatingly unfavourable for human and economic wellbeing. An estimated one hundred million people killed in the twentieth century, one billion set to be killed in the twenty-first century, US$1.4 trillion annually lost to the global economy – these are the preconditions for the maintenance of their market value and over US$50 billion in combined annual profit (Drope et al. 2018; Goodchild et al. 2017). Over the century, the bulk of this individual and economic ruin is set to be inflicted upon LMICs least able to absorb the economic and fiscal burden of tobacco use (Drope et al. 2018; CTFK 2018). Meanwhile, most of the profit will flow back to the high-value end of the production process – marketing and innovation – that is predominately located in HICs and tobacco industry’s shareholders who are also predominately located in HICs (CTFK 2018).
But past successes in defying the tobacco industry and bending the curve of the epidemic show how the projections – one billion lives lost, economic development stalled – can be defied and tobacco industry further outmanoeuvred. The WHO FCTC is a proven success and its provisions are impactful when implemented. At present, 90% of the world’s population is covered by it and most of the world’s population is covered by one of its demand reduction measures at a best practice level, as set out in the MPOWER technical package (WHO 2019a). It is this targeted and supported implementation of the WHO FCTC that turned the tide on the global epidemic – with the total number of male tobacco users finally peaking in 2018 (WHO 2019b). This widespread implementation was made possible by the Convention Secretariat and WHO assistance to States Parties, along with academic and civil society partners around the world, making their own innovative and concerted attempts to realise the WHO FCTC’s aspirations. Particularly crucial was the packaging of the WHO FCTC’s demand reduction measures into the digestible MPOWER technical package that was coupled, due to the multisectoral assistance of the Bloomberg Philanthropies’ Global Initiative to Reduce Tobacco Use, with granular implementation tracking and tobacco use surveillance. This ensured opportunities for mutual review and provided evidence on best practice in implementation. Efforts to protect tobacco control policymaking from industry interference were, although never complete, also key to the WHO FCTC’s successes. Without at least partial implementation of Article 5.3 and the COP Guidelines to it, industry’s advantages in disrupting and undermining tobacco control processes would have been only greater yet. National initiatives enshrining both the article and its guidelines have often preceded and accompanied effective tobacco control (Assunta 2018). In a similar way, the UN Interagency Task Force on NCDs, which has both the WHO and the Convention Secretariat as leading participants, has crafted a strong policy to prevent industry tactics operating in the UN and then ensured its implementation at the intergovernmental level (UN Interagency Taskforce 2020; Zhou and Liberman 2018). Opposition to industry tactics has been supported by WHO’s collaborating centres and the Convention Secretariat’s knowledge hubs and monitoring centres, established through essential bilateral partnerships with research institutes and academia. Independently of WHO and the Convention Secretariat, these efforts are also facilitated by key CSOs involved in preventing and understanding industry interference. These cross-cutting global multisectoral networks for anticipating and counteracting industry interference provide a blueprint for the scaled-up action needed as tobacco industry tactics continue to evolve in the years ahead.
This evolution of tobacco industry tactics represents the most significant challenge to the acceleration of WHO FCTC implementation needed to achieve SDG 3.A and prevent the epidemic from plateauing in middle-income countries and escalating in less affected low-income countries. In LMICs there is a need to counter conventional tobacco industry interference such as CSR used to gain a foothold in policymaking, scare tactics to undermine, and preempt effective tobacco taxation and flagrant evasion of tobacco control regulations when enforcement is insufficient. At the same time, in all countries, the tobacco industry continues to obstruct tobacco product regulation and has escalated its use of litigation before domestic and international tribunals to defeat, delay, or at least disincentivise effective tobacco control measures. Although the WHO FCTC and the COP’s guidelines have proven themselves highly effective as a component of a litigation defence strategy for alleged breaches of domestic or international obligations, the industry has also proven itself capable of leveraging the perceived threat of litigation defeat and the resources needed to defend against a challenge in order to shift the political economy of tobacco control against effective measures (Zhou et al. 2019; McGrady 2018). In HICs and some upper-middle income countries, meanwhile, the “harm reduction” façade behind which industry has been seeking to expand the nicotine market while rehabilitating its public image is causing the perception of fracture in the tobacco control community and is permitting industry to circumvent tobacco control regulations. These evolving and emerging challenges by industry to tobacco control need to be addressed with the same playbook of multi-level, multisectoral, whole-of-government networked collaboration drawing on evidence-based measures and evidence of best practice in implementation as needed for the more fundamental issue of insufficient acceleration in WHO FCTC implementation.
Tobacco Control in the Post-COVID-19 Era
A sense of shame for being responsible for deadly products that has killed millions of people might have dictated reticence, if not penitence, as COVID-19, a communicable disease causing lower respiratory infection and damage to the cardiovascular system, spread through a global population whose lungs and hearts have been weakened by smoking (Mehra et al. 2020; Kluge et al. 2020; WHO 2020). But the tobacco industry is not one to waste a crisis and to miss an opportunity and has instead initiated a charm offensive alongside a campaign of mass-deception. To burnish their image in the face of a rising death toll attributable to their products as a COVID-19 comorbidity, industry has, for example, created a COVID-19 relief fund in India, donated respirators in Greece and provided funds for respirators, test kits and protective equipment in Romania (Gilmore and Branston 2020). At the same time, industry has lobbied to keep their factories operational in New Zealand and the United States – with the former granting a tobacco factory status as an essential business eligible to remain operational during a tight lockdown (Gilmore and Branston 2020).
A more brazen campaign against the science has seen industry, through its affiliates, attempt to muddy the waters on the link between tobacco-related disease and severe outcomes in COVID-19 progression (GGTC 2020). They have even gone so far as to seize upon weak clinical studies and misuse descriptive epidemiological studies to claim nicotine acts has a prophylactic effect for COVID-19 (GGTC 2020; WHO 2020b). This has then been followed-up with intense marketing by tobacco industry of their novel and emerging nicotine and tobacco products (GGTC 2020). Despite irresponsible amplification of these claims in the media, available evidence is unable to confirm any role for tobacco or nicotine in the prevention or treatment of COVID-19 (WHO 2020). Any claim to the contrary is promotion of an unproven intervention (WHO 2020).
Given clear evidence that tobacco-related disease exacerbates the risk of severe outcomes of COVID-19, the pandemic and its economic fallout are an opportunity to shift newly health conscious and price conscious tobacco users toward quitting and discourage never-smokers and youth away from initiation (Gilmore and Branston 2020; WHO 2020). To seize this opportunity, WHO FCTC implementation using the MPOWER technical package will need to be scaled up with a focus on tobacco tax rises and tobacco cessation services. The case for tax rises has never been clearer, as the need to finance COVID-19 responses and support strained healthcare systems in the context of declining economies is prompting policymakers to turn toward the use of scaled up tobacco excise (Gilmore and Branston 2020). Providing proven and evidence-based cessation services, such as funded quit-lines and nicotine patches, at this time is also critical to ensure that current tobacco users are supported in quitting (Ghebreyesus 2019; WHO 2020). At the same time WHO, the Convention Secretariat and all tobacco control advocates will need to cooperate to anticipate and counteract tobacco industry obfuscation over their product’s link to severe outcomes and their attempt to market their novel tobacco products, HTPs, as cessation devices (Gilmore and Branston 2020; WHO 2020). Caution also needs to be shown toward industry and industry affiliate attempts to divert users to ENDS and ENNDS and thereby retain them in the nicotine market (WHO 2020).
The WHO FCTC as Best Practice Example
The WHO FCTC was a pathfinder for the trend away from one-way North-South and donor-driven power dynamics and toward the centring of LMICs within frameworks of universal applicability that also explicitly engage with equity and human rights. Accordingly, it is unsurprising that the WHO FCTC’s importance is affirmed in the SDGs and the three UN General Assembly political declarations on NCDs. Nor is it surprising that the UN Committee on the Rights of the Child has linked the child’s right to health with its implementation, that the UN Committee on the Elimination of Discrimination Against Women has connected freedom from sex-based discrimination with its gender-sensitive implementation, or that there is increasing recognition that the production and marketing of tobacco is irreconcilable with the human right to health (Bettcher et al. 2015; Zhou and Liberman 2018; Burci 2018). This cross-cutting and multisectoral influence can also be seen in how the WHO FCTC has had significant influence across the disputes and fora of international legal regimes on human rights, trade, investment, and intellectual property (Zhou and Liberman 2018). This influence in the regimes of international human rights law and international economic law is not, however, restricted to tobacco. By setting a precedent for the recognition of the commercial determinants of health paradigm in favour of the individual responsibility paradigm, the WHO FCTC is shifting the balance in favour of the right to regulate to protect human health from key risk factors for NCDs (Burci 2018).
There have also been frequent calls to follow the path of the WHO FCTC more exactly through the adoption of further Conventions on NCDs generally or on specific risk factors such as alcohol use or nutrition (Burci 2018). This is a recognition of how the WHO FCTC has impelled implementation at the national level, rallied the support among networks of supporters, and won tobacco control recognition as a paramount value in domestic and international legal regimes (Burci 2018). Given the increasing burden of all NCDs and risk factors among LMICs, these calls have merit but their opponents – the multinational alcohol, food, and beverage industries – are, in many respects, more influential and much less disgraced than the tobacco industry was in the late 1990s and remains today (Burci 2018). The trends in the international community since the adoption of the WHO FCTC have also been away from the use of hard-law binding treaties and toward more flexible instruments (Burci 2018). There is, however, potential for this trend to shift as the COVID-19 pandemic has shone a spotlight on the vulnerabilities created by negative commercial determinants of health, unhealthy consumption, and the burden of NCDs.
Even in the absence of moves toward a binding convention on any of these other principal NCD risk factors, the WHO FCTC can still act as a pathfinder for action. This is because only half the story of the WHO FCTC’s success lies in its legally binding nature. As we have seen, much of its success has derived from the firm grounding in evidence of all its provisions and guidelines as well as the way key provisions have been highlighted and packaged in MPOWER and the networks of support in implementation provided by other intergovernmental bodies, philanthrophies, and CSOs. Crucially, there is a need to address the vector of these epidemics – multinational industries predominately based in HICs – by using the playbook of containment and surveillance taken in the successful tobacco control effort. Although there is a tendency toward cooperative relationships with alcohol, food, and beverage industries, this should not obscure the fact that they adopt many of the same tactics used by tobacco industry to influence and globalise negative commercial determinants of health (McInerney 2019).
References
Assunta M (2018) Good country practices in the implementation of WHO FCTC article 5.3 and its guidelines. WHO FCTC Secretariat, Geneva. Available at https://www.who.int/fctc/publications/fctc-article-5-3-best-practices.pdf?ua=1
Bettcher D, Yach D, Guindon GE (2000) Global trade and health: key linkages and future challenges. Bull World Health Organ 78(4):521–534
Bettcher D, DeLand K, Lien G, Gonzalez-Martinez F, Huvos A, Solomon S, Schwerdtfeger U, Nikogosian H, Tritscher A, Dalzell J (2015) International efforts to promote public health. In: Detels R, Gulliford M, Karim QA, Tan CC (eds) Oxford textbook of public health, 6th edn. Oxford University Press, Oxford. https://doi.org/10.1093/med/9780199661756.001.0001
Bialous SA (2019) Impact of implementation of the WHO FCTC on the tobacco industry’s behaviour. Tob Control 28:s94–s96
Bialous SA, Glantz SA (2018) Heated tobacco products: another tobacco industry global strategy to slow progress in tobacco control. Tob Control 27:s111–s117
Burci GL (2018) Global health law: present and future. In: Burci GL, Toebes B (eds) Research handbook on global health law. Edward Elgar Publishing, Cheltenham, pp 486–528
Campaign for Tobacco Free Kids (CTFK) (2018) Who is profiting from tobacco? A closer look at the shareholders of multinational tobacco companies and their subsidiaries. Available via CTFK. https://www.tobaccofreekids.org/assets/content/press_office/2018/WhosProfitingFromTobacco.pdf. Accessed 10 Dec 2019
Centre for Tobacco Control in Africa (2020) About us. https://ctc-africa.org/africamap/#. Accessed 20 Jun 2020
Chung-Hall J, Craig L, Gravely S, Sansone N, Fong GT (2018) Impact of the WHO FCTC over the first decade: a global evidence review prepared for the Impact Assessment Expert Group. Tob Control 28:s119–s128
Crosbie E, Glantz SA (2014) Tobacco industry argues domestic trademark laws and international treaties preclude cigarette health warning labels, despite consistent legal advice that the argument is invalid. Tob Control 23:e7–e16
CTFK (2020 Updated Feb 10). Standardised or plain tobacco packaging: international developments. Available via www.tobaccofreekids.com. Accessed 20 Feb 2020
Drope J, Schluger NW, Cahn Z, Drope J, Gomeshtapeh FI, Liber A, Nargis N, Stoklosa M (2018) The tobacco atlas, 5th edn. American Cancer Society, Vital Strategies, Atlanta. www.tobaccoatlas.org. Accessed 20 Dec 2019
Eckhardt J, Holden C, Callard C (2016) Tobacco control and the World Trade Organization: mapping member states’ positions after the framework convention on tobacco control. Tob Control 26(6):692–698
Evan-Reeves K, Gilmore A, Zatonski M, Peeters S, Matthes BK, Hiscock R, Lauber K, Legg T (2020) Addiction at any cost: Phillip Morris international uncovered. Available via Vital Strategies. https://exposetobacco.org/wp-content/uploads/STOP_Report_Addiction-At-Any-Cost.pdf. Accessed 10 Apr 2020
GBD 2015 Tobacco Collaborators (2017) Smoking prevalence and attributable disease burden in 195 countries and territories, 1990–2015: a systematic analysis from the Global Burden of Disease Study 2015. Lancet 389:1885–1906. https://doi.org/10.1016/S0140-6736(17)30819-X
Ghebreyesus T (2019) Progress in beating the tobacco epidemic. Lancet. https://doi.org/10.1016/S0140-6736(19)31730-1. Accessed 30 Jul 2019
Gilmore AB, Branston JR (2020) Phillip Morris international: the beginning of the end? Available via STOP. https://exposetobacco.org/news/pmi-agm/. Accessed 15 May 2020
Gilmore AB, Fooks G, Drope J, Bialous SA, Jackson RR (2015) Exposing and addressing tobacco industry conduct in low-income and middle-income countries. Lancet 385:1029–1043
Global Centre for Good Governance in Tobacco Control (GGTC) (2020) How governments can use the WHO FCTC to counter tobacco industry tactics and maximize public health during the COVID-19 pandemic. Available via Stopping Tobacco Organizations & Products (STOP). https://exposetobacco.org/wp-content/uploads/STOP_COVID19_Policy_Brief_Final.pdf. Accessed 15 Jun 2020
Goodchild M, Nargis N, d’Espaignet ET (2017) Global economic cost of smoking-attributable diseases. Tob Control 27:58–64
International Mayors Forum (2016) Shanghai consensus on health cities. Healthy Cities Mayors Forum, Shanghai. Available via WHO. https://www.who.int/healthpromotion/conferences/9gchp/9gchp-mayors-consensus-healthy-cities.pdf?ua=1. Accessed 27 Jun 2020
Jannsen F (2019) Similarities and differences between sexes and countries in the mortality imprint of the smoking epidemic in 34 low-mortality countries, 1950–2014. Nicotine Tob Res:1–11. https://doi.org/10.1093/ntr/ntz154
Kickbusch I, Allen L, Franz C (2016) The commercial determinants of health. Lancet 4:e895–e896
Kluge HHP, Wickramasinghe K, Rippin HL, Mendes R, Peters DH, Kontsevaya A, Breda J (2020) Prevention and control of non-communicable diseases in the COVID-19 response. Lancet. https://doi.org/10.1016/S0140-6736(20)31067-9
Krug E, Bettcher D, Arnold V, Robinson S (2019) The role of cities in preventing non-communicable diseases and road injuries. Public Health Panorama 5(2–3):123–367
Lee K (2008) Global institutions: the World Health Organization. Routledge, Abingdon
Levy DT, Yuan Z, Lou Y, Mays D (2018) Seven years of progress in tobacco control: an evaluation of the effect of nations meeting the highest level MPOWER measures between 2007 and 2014. Tob Control 27:50–57. https://doi.org/10.1136/tobaccocontrol-2016-053381
Mamudu HM, Glantz SA (2009) Civil society and the negotiation of the Framework Convention on Tobacco Control. Glob Public Health 4(2):150–168. https://doi.org/10.1080/17441690802095355
Mamudu HM, Hammond R, Glantz SA (2008) Project Cerberus: tobacco industry strategy to create an alternative to the Framework Convention on Tobacco Control. Am J Public Health 98(9):1630–1642
Mamudu HM, Hammond R, Glantz SA (2011) International trade versus public health during the FCTC negotiations, 1999–2003. Tob Control 20:e3–e13. https://doi.org/10.1136/tc.2009.035352
Marquez PV, Moreno-Dodson B (2017) Tobacco tax reform: at the crossroads of health and development. World Bank, Washington, DC. https://openknowledge.worldbank.org/handle/10986/28494
McGrady B (2018) Health and international trade law. In: Burci GL, Toebes B (eds) Research handbook on global health law. Edward Elgar Publishing, Cheltenham, pp 104–134
McInerney TF (2019) The WHO FCTC and global governance: effects and implications for future global public health instruments. Tob Control 28:s89–s93. https://doi.org/10.1136/tobaccocontrol-2018-054358
Mehra MR, Desai SS, Kuy SR, Hendry TD, Patel AN (2020) Cardiovascular disease, drug therapy, and mortality in Covid-19. N Engl J Med. https://doi.org/10.1056/NEJMoa2007621
Minhas R, Bettcher D (2010) WHO – coordinating international tobacco control. In: Boyle P, Gray N, Henningfield J, Seffrin J, Zatonski W (eds) Tobacco: science, policy and public health. Available via Oxford Scholarships online. https://doi.org/10.1093/acprof:oso/9780199566655.003.0043.
Moodie R, Stuckler D, Monteiro C, Sheron N, Neal B, Thamarangsi T, Lincoln P, Casswell S (2013) Profits and pandemics: prevention of harmful effects of tobacco, alcohol, and ultra-processed food and drink industries. Lancet 381:670–679. https://doi.org/10.1016/S0140-6736(12)62089-3
Nikogosian H, Kickbusch I (2018) Interface of health and trade: a viewpoint from health diplomacy. BMJ Gob Health 3. https://doi.org/10.1136/bmjgh-2017-000491
Panel Report, GATT 1947 (1990) Thailand – restrictions on importation of and internal taxes on cigarettes. DS10/R – 37S/200
Philip Morris Brand Sàrl (Switzerland), Philip Morris Products S.A. (Switzerland), Abal Hermanos S.A. (Uruguay) v. Oriental Republic of Uruguay (2016) ICSID case no. ARB/10/7. https://www.italaw.com/cases/460. Accessed 5 Dec 2019
Reubi BV (2016) The internationalisation of tobacco control, 1950–2010. Med Hist 60(4):453–472. https://doi.org/10.1017/mdh.2016.97
Reynolds LA, Tansey EM (eds) (2010) WHO Framework Convention on Tobacco Control. Wellcome witnesses to twentieth-century medicine 43, Queen Mary, University of London, London
Roemer R, Taylor A, Larviviere J (2005) Origins of the WHO Framework Convention on Tobacco Control. Am J Public Health 96(6):936–938
Rojhani A, Hung C, Chew S, Honeysett C, Mullin S, Karpati A (2019) The Partnership for Health Cities: activating urban governments as engines of public health practice. In: Galea S, Ettman CK, Vlahov D (eds) Urban health. Available via Oxford Scholarships online. https://doi.org/10.1093/oso/9780190915858.001.0001. Accessed 25 Jan 2020
The Lancet (2019) E-cigarettes: time to realign our approach? Lancet 394:1297
Thun MJ, Freedman ND (2017) Tobacco. In: Thun M, Linet MS, Cerhan JR, Haiman CA, Schottenfeld D (eds) Cancer epidemiology and prevention. Available via Oxford Scholarship online. https://doi.org/10.1093/oso/9780190238667.003.0011
United Nations Inter-Agency Task Force on the Prevention and Control of Non-communicable Diseases (2020) Report of the Director-General of the World Health Organization on the United Nations Inter-Agency Task Force on the prevention and control of non-communicable diseases. Available via United Nations Economic and Social Council. https://undocs.org/E/2020/51
US Department of Health and Human Services (US HSS) (2014) The health consequences of smoking: 50 years of progress. A report of the Surgeon General. US Department of Health and Human Services, Atlanta. Available via National Centre for Biotechnology Information. https://www.ncbi.nlm.nih.gov/books/NBK179276/pdf/Bookshelf_NBK179276.pdf
US National Cancer Institute and World Health Organization (NCI and WHO) (2016) The economics of tobacco and tobacco control. National Cancer Institute Tobacco Control Monograph 21. http://cancercontrol.cancer.gov/brp/tcrb/monographs/21/index.html
Vital Strategies (2019) Crooked nine: nine ways the tobacco industry undermines health policy. New York. Available via STOP. https://exposetobacco.org/wp-content/uploads/2019/09/Crooked-9-STOP.pdf. Accessed 10 Mar 2020
WHO (2008) A policy package to reverse the tobacco epidemic: MPOWER. Geneva. https://apps.who.int/iris/bitstream/handle/10665/43888/9789241596633_eng.pdf?sequence=1&isAllowed=y
WHO (2010) Gender, women, and the tobacco epidemic. Geneva. https://www.who.int/tobacco/publications/gender/women_tob_epidemic/en/
WHO (2013) Report on the global tobacco epidemic, 2013. Geneva. https://www.who.int/tobacco/global_report/2013/en/
WHO (2017) Report on the global tobacco epidemic, 2017. Geneva. https://www.who.int/tobacco/global_report/2017/en/
WHO (2018a) Tobacco product regulation: basic handbook. Geneva. https://www.who.int/tobacco/publications/prod_regulation/basic-handbook/en/
WHO (2018b) Noncommunicable disease country profiles. Geneva. https://apps.who.int/iris/handle/10665/274512
WHO (2018c) Saving lives, spending less: a strategic response to noncommunicable diseases. Geneva, WHO/NMH/NVI/188. https://apps.who.int/iris/rest/bitstreams/1137198/retrieve
WHO (2019a) Report on the global tobacco epidemic, 2019. Geneva. https://www.who.int/tobacco/global_report/en/
WHO (2019b) Global report on trends in prevalence of tobacco use 2000–2025, 3rd edn, Geneva. https://www.who.int/publications/i/item/who-global-report-on-trends-in-prevalence-of-tobacco-use-2000-2025-third-edition
WHO (2019c) Stronger collaboration, better health: global action plan for healthy lives and well-being for all. Geneva. https://www.who.int/publications/i/item/stronger-collaboration-better-health-global-action-plan-for-healthy-lives-and-well-being-for-all
WHO (2019d) Thirteenth global programme of work 2019–2023, Geneva. https://apps.who.int/iris/bitstream/handle/10665/324775/WHO-PRP-18.1-eng.pdf?ua=1
WHO (2019e) The power of cities: tackling noncommunicable diseases and road traffic injuries. Geneva, WHO/NMH/PND/2019. https://www.who.int/ncds/publications/tackling-ncds-in-cities/en/
WHO (2019f) WHO presence in countries, territories, and areas: 2019 report, Geneva. https://www.who.int/country-cooperation/publications/who-presence-report-2019/en/
WHO (2020) WHO statement: tobacco use and COVID-19. Geneva. https://www.who.int/news-room/detail/11-05-2020-who-statement-tobacco-use-and-covid-19. Accessed 12 May 2020
WHO FCTC COP (2007) Guidelines for implementation of Article 5.3. Decision FCTC/COP3(7)-https://www.who.int/fctc/guidelines/article_5_3.pdf?ua=1
WHO FCTC COP (2008a) Guidelines for implementation of Article 11. Decision FCTC/COP3(10). https://www.who.int/fctc/guidelines/article_11.pdf?ua=1
WHO FCTC COP (2008b) Guidelines for implementation of Article 13. Decision FCTC/COP3(12). https://www.who.int/fctc/guidelines/article_13.pdf?ua=1
WHO FCTC COP (2014) Guidelines for implementation of Article 6. Decision FCTC/COP6(5). https://apps.who.int/iris/bitstream/handle/10665/145110/FCTC_COP6%285%29-en.pdf?sequence=1&isAllowed=y
Wipfli H, Samet JM (2016) One hundred years in the making: the global tobacco epidemic. Annu Rev Public Health 37:149–166. https://doi.org/10.1146/annurev-publhealth-032315-021850
World Bank (1999) Curbing the epidemic: governments and the economics of tobacco control. Washington, DC. http://documents.worldbank.org/curated/en/914041468176678949/pdf/multi-page.pdf
WTO Appellate Body (2020) Australia – certain measures concerning trademarks, geographical indications and other plain packaging requirements applicable to tobacco products and packaging. World Trade Organization, Geneva, pp 20–4018. https://www.wto.org/english/tratop_e/dispu_e/435_441abr_e.pdf
WTO Panel (2018) Australia – certain measures concerning trademarks, geographical indications and other plain packaging requirements applicable to tobacco products and packaging. World Trade Organization, Geneva, pp 18–4061. https://www.wto.org/english/tratop_e/dispu_e/cases_e/ds467_e.htm
Zhou S, Liberman J (2018) The global tobacco epidemic and the WHO Framework Convention on Tobacco Control – the contributions of the WHO’s first convention to global health law and governance. In: Burci GL, Toebes B (eds) Research handbook on global health law. Edward Elgar Publishing, Cheltenham, pp 340–388
Zhou SY, Liberman JD, Ricafort E (2019) The impact of the WHO Framework Convention on Tobacco Control in defending legal challenges to tobacco control measures. Tob Control 28:s133–s118. https://doi.org/10.1136/tobaccocontrol-2018-054329